











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Case Description
We report the case of a 31-year-old female patient with a history of thoracolumbar scoliosis surgically corrected via thoracolumbar arthrodesis. Over the preceding six months, she experienced occasional low back pain refractory to conservative management with physiotherapy, prompting imaging evaluation of the lumbosacral spine and sacroiliac joints.
MRI (Fig.1) revealed an incidental nodule on the posterior aspect of the S1 vertebral body. The lesion was well-defined, regular, and measured 30 mm, with heterogeneous T2 hyperintensity and T1 hypointensity. No evidence of intralesional fat, surrounding edema, diffusion restriction, or post-contrast enhancement were observed.
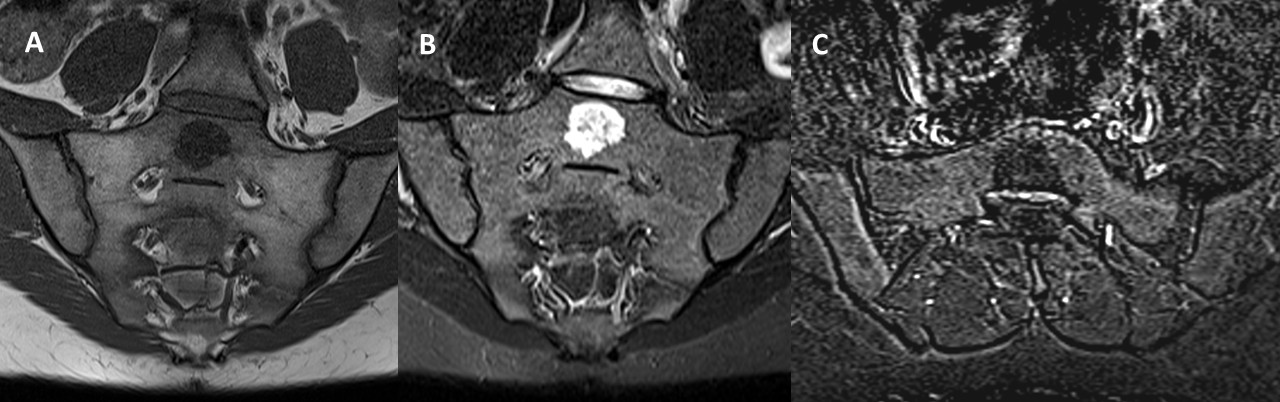
Figure 1: Coronal oblique T1-weighted (A), STIR (B) and axial oblique T1 fat saturated post-contrast subtraction (C) MRI images demonstrate a lesion in the midline of the S1 vertebral body with heterogeneous T2 hyperintensity and T1 hypointensity. No evidence of post-contrast enhancement or surrounding edema was observed.
Subsequent CT of the lumbosacral spine (Fig.2) demonstrated a mild osteosclerotic lesion with poorly defined margins with preservation of the trabecular bone pattern. No radiological signs of aggressiveness, such as bone destruction or soft tissue involvement were observed.
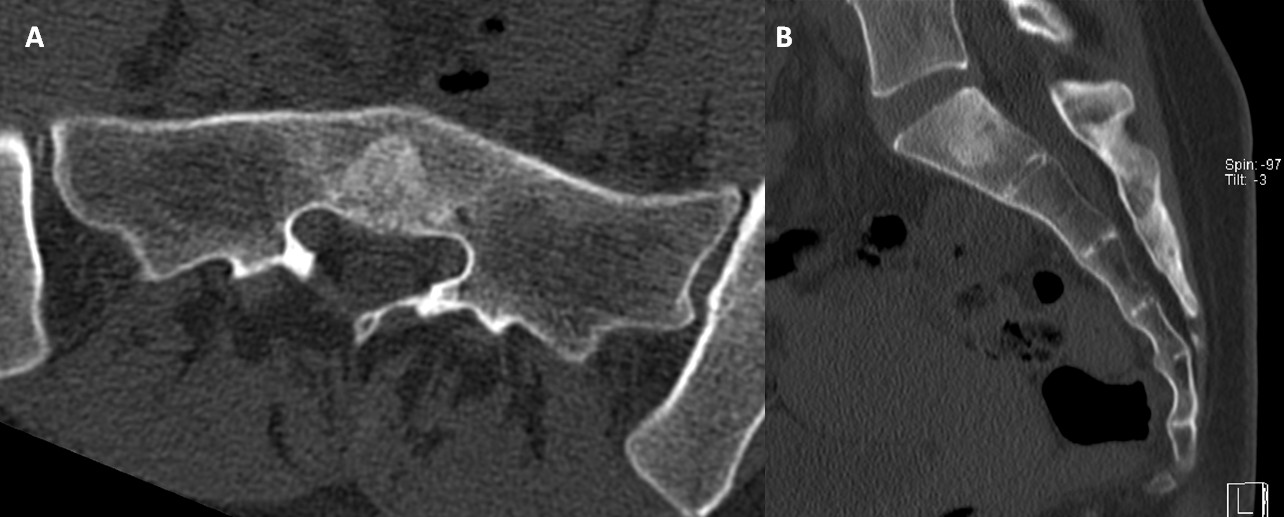
Figure 2: Axial (A) and Sagittal (B) CT images of the lumbosacral spine show a mild osteosclerotic lesion in the midline of the S1 vertebral body, with poorly defined margins and preservation of the trabecular bone pattern. No evidence of bone destruction or soft tissue involvement is observed.
The sacroiliac joints appeared normal on both MRI and CT, with no additional findings of inflammatory or degenerative changes or complications related to the surgical instrumentation observed.
Given the imaging characteristics, the lesion was categorized as Bone-RADS 3 (indeterminate lesion, requiring imaging follow-up). A decision was made to opt for imaging surveillance rather than an anatomopathological study, considering the absence of aggressive features and the need to assess its stability over time.
Discussion
Benign notochordal cell tumors (BNCTs) are rare lesions derived from remnants of the notochord and are typically discovered incidentally. Although their precise prevalence is unclear, autopsy studies suggest they may occur in up to 20% of the population, highlighting their relatively common presence as incidental findings in asymptomatic individuals.1,2
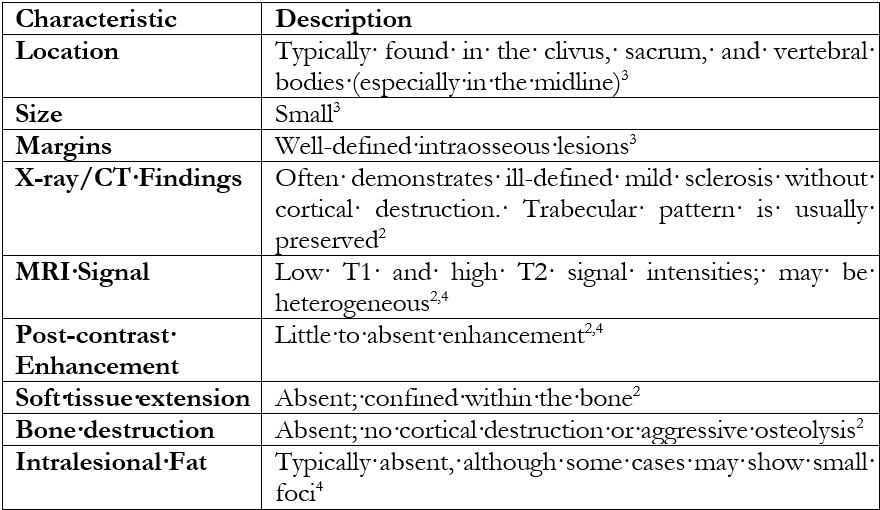
They are distinct from chordomas, with which they share embryological origins, but differ in clinical behavior and prognosis3,4 BNCTs are most commonly found in the clivus and sacrum, presenting as small, well-defined intraosseous lesions.3 Radiographically, they exhibit mild sclerosis without cortical destruction or soft tissue extension.1,4 MRI findings include low T1 and high T2 signal intensities, with little or no enhancement post-contrast.2,4. In contrast, chordomas are aggressive, osteolytic, and often associated with significant soft tissue masses.(Table 1)3,4
BNCTs are considered benign lesions that do not require surgical resection.4 However, sporadic cases associated with chordoma have been reported in the literature, and it remains controversial whether these are concomitant lesions or if BNCT may occasionally act as a precursor to chordoma.3,4 That being said, most sources recommend imaging follow-up to confirm their radiological stability and rule out malignant progression, although they do not specify the optimal follow-up interval.3,4,5

