











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Case Presentation
We present a case of a 65-year-old male that presented to the emergency department due to a 3-day history of vomiting and abdominal pain. He also complained of postprandial fullness, anorexia, and weight loss in the past 3 months. He had a history of cholelithiasis and was on the waiting list for cholecystectomy. On examination, he had a distended, tender abdomen in the upper quadrants and right iliac fossa. Laboratory test results showed a mild neutrophilic leukocytosis, anemia, and C-reactive protein of 3.99 mg/dL (normal range <0.5 mg/dL). Abdominal ultrasound performed in the emergency department showed multiple hypodense hepatic nodules, cholelithiasis without signs of cholecystitis and heterogeneous intragastric content. Subsequently, he performed a CT abdominal scan which showed large gallstones impacted in the duodenum, causing gastric outlet obstruction (Bouveret’s syndrome). It also suggested the presence of a cholecystoduodenal fistula (Figure 1). No dilation of small bowel loops or any intraluminal content was identified. He was admitted for additional study. For better characterization of the liver lesions, an abdominal MRI was performed, characterizing the liver nodules as hemangiomas. Also, several dilated fluid-filled small bowel loops could now be observed, and a large gallstone was found in the ileum, suggesting migration of one of the previously identified in the duodenum on the initial CT scan. In the stomach, another gallstone could be identified. (Figure 2). Esophagogastroduodenoscopy showed one large black stone of 6-7cm in the distal antrum. The patient underwent an exploratory laparotomy with intra-abdominal examination, and two stones were identified, one at the gastric level and the other at the distal ileum, close to the ileocecal valve. Gastrolithotomy and enterolithotomy were performed with stone removal. The patient recovery was unremarkable.
Gallstone ileus is a rare complication in patients with cholelithiasis. It’s commonly associated with small bowel obstruction. In patients with intestinal obstruction, this clinical entity is the cause in 1 to 4% of cases. It generally occurs after the development of a fistula between the gallbladder and small bowel, the majority located in duodenum. It’s more common in female patients, in the elderly and in patients with multiple comorbidities. The majority of stones are impacted in the distal ileum and ileocecal valve, which account for 60-85% of cases, because of their relatively narrow lumen and less active peristalsis.1,2,3The most frequent clinical presentation is with symptoms of small bowel obstruction. In the clinical setting of bowel perforation, patients present with systemic signs and symptoms. Diagnosis is made with abdominal x-ray, CT-scan, ultrasonography, or MR cholangiopancreatography.4 Proximal obstruction of the gastric outlet or duodenum occurs rarely (4%) and is known as Bouveret syndrome, a rare form of gallstone ileus. The stone migrates through a cholecystogastric or cholecystoduodenal fistula. Bouveret syndrome represents ~1%-3% of cases of gallstone ileus. Bouveret’s syndrome imagiological workup is similar to distal obstructions.5 The cornerstone treatment of gallstone ileus, including Bouveret’s syndrome, is surgical removal of the gallstone (enterolithotomy or bowel resection), cholecystectomy and fistulae closure. Mortality rates revealed considerable reductions in the past years, to current rates of less than 7%.6
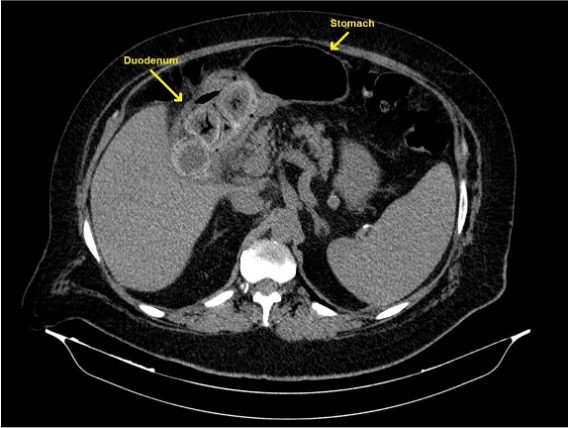
Figure 1: Unenhanced axial CT slice showing large gallstones impacted in the duodenum, causing gastric outlet obstruction (Bouveret syndrome). The gallbladder was contracted, suggesting that a cholecystoduodenal fistula had been formed, from which the stones passed to the duodenum.
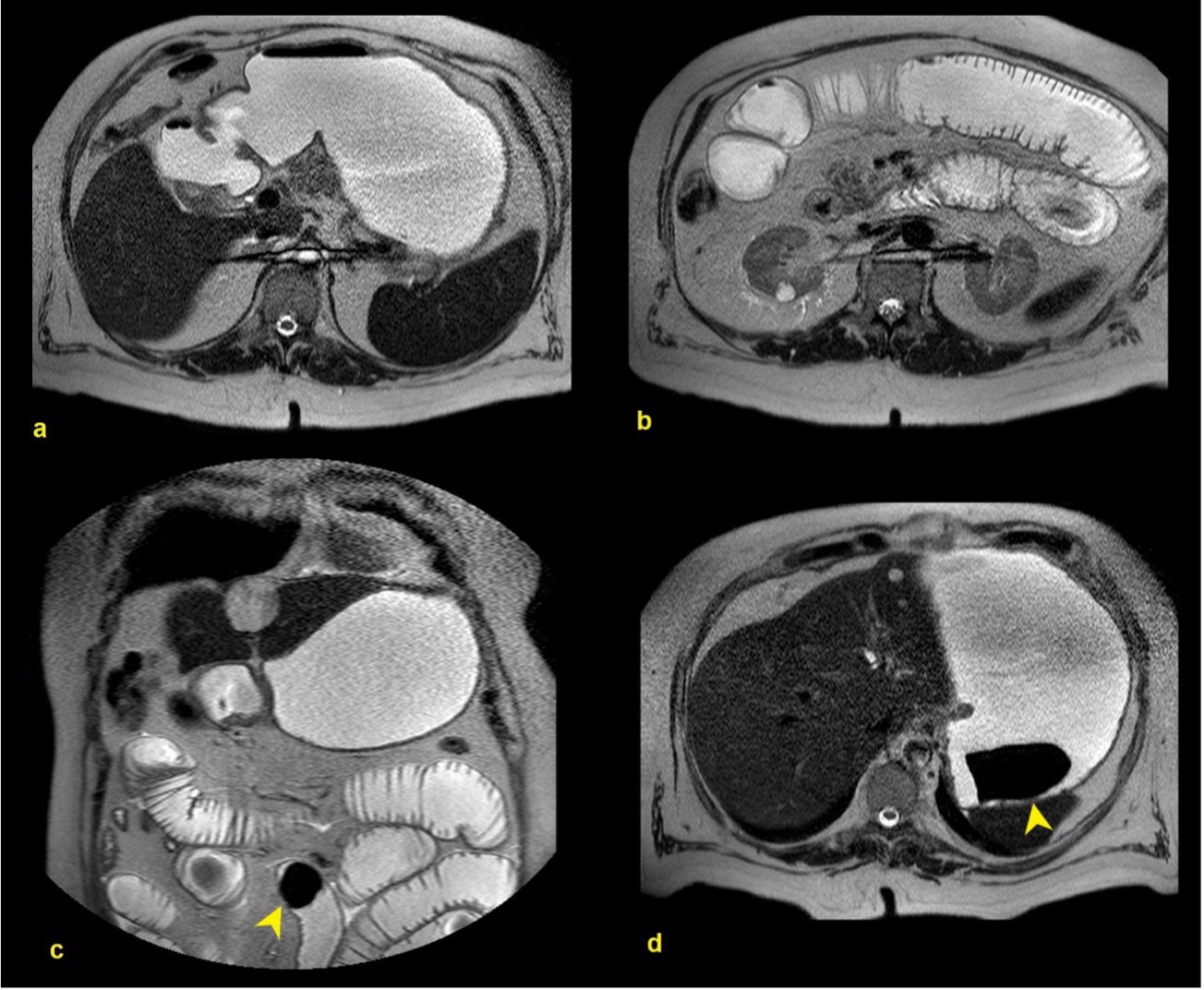
Figure 2: T2-weighted axial (a, b, d) and coronal (c) images of an MRI performed one week later. No gallstones were identified in the duodenum (a). Instead, several dilated fluid-filled small bowel loops could now be observed (b). Even though the MRI did not include the pelvis, the cause of the obstruction was a large gallstone that was found in the ileum (c, arrowhead). Another gallstone could be observed in the stomach (d, arrowhead).

