











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Images in Case
A 43-year-old man reported a painless enlarging right periareolar lump noticed two years earlier. Physical examination showed a well-circumscribed, mobile, subareolar mass; skin and nipple were normal and no axillary lymph-nodes were palpable.
Bilateral mammography demonstrated an oval, sharply marginated lesion measuring 25 × 8 mm in the right retro-areolar region (Fig. 1). Its interior displayed an admixture of radiolucent fat and radiodense fibroglandular tissue, producing the characteristic “breast-within-a-breast” pattern; a faint delimiting rim was suggested around the mass. The left breast was fatty (BI-RADS 1).
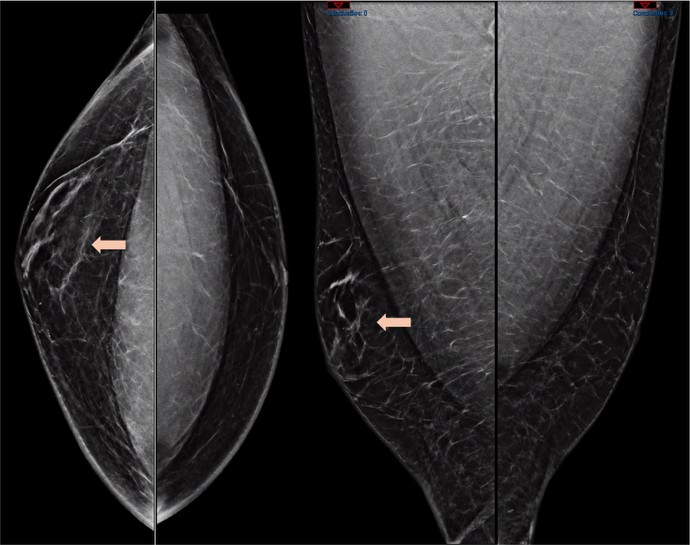
Figure 1: Bilateral craniocaudal and mediolateral-oblique mammograms. In the right breast, an oval periareolar mass (arrow) is circumscribed by a faint capsule; the mixture of radiolucent fat and radiodense fibroglandular tissue produces the characteristic “breast-within-a-breast” appearance.
Ultrasound confirmed an encapsulated, oval, heterogeneous lesion parallel to the skin (Fig. 2A). Intermingled hyperechoic (fibroglandular) and hypoechoic (fatty) foci were seen, bound by an echogenic rim; Doppler showed no internal vascularity. A measurement view (Fig. 2B) documented a maximum length of 25 mm and underscored the lesion’s smooth capsule and mixed fibroglandular-fat composition.
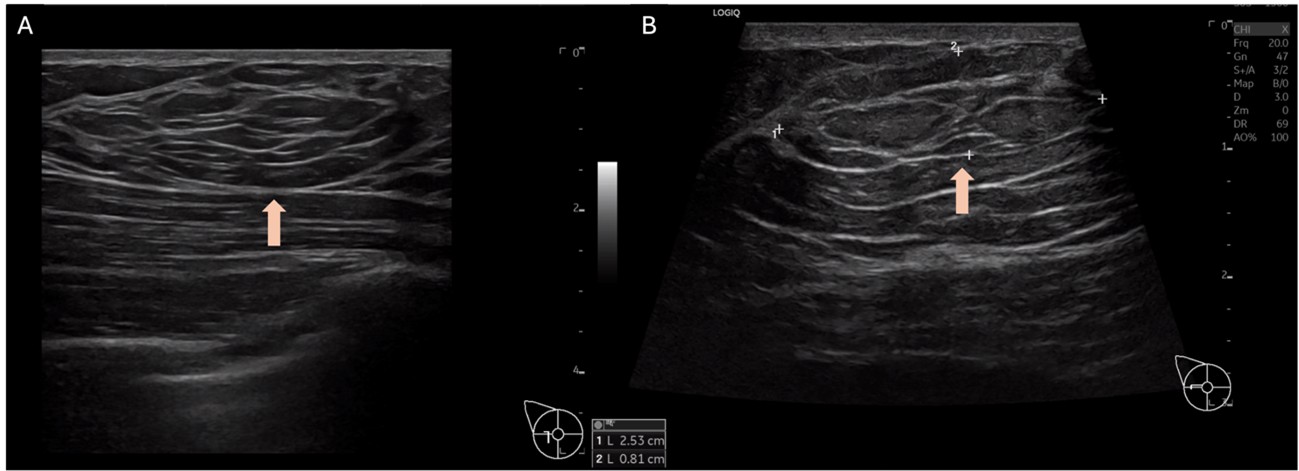
Figure 2: Ultrasound images of the right breast hamartoma. (A) Radial view: an encapsulated oval lesion (arrow) with heterogeneous echotexture-intermixed hyperechoic fibroglandular tissue and hypoechoic fat-lying parallel to the skin, without posterior shadowing or internal Doppler flow. (B) Long-axis measurement view confirms a maximal length of 25 mm (arrow) and better delineates the smooth echogenic capsule and the mixed fibroglandular-fat composition.
The imaging constellation matched textbook criteria for hamartoma, so the lesion was categorised BI-RADS 2 (benign); biopsy was deemed unnecessary. Annual clinical review was advised, reserving repeat imaging for growth or new symptoms.
Discussion
Breast hamartoma corresponds to a disorganised but benign aggregation of mammary fat and fibroglandular tissue within a pseudocapsule. Although it represents up to 1 % of benign breast tumours in women, it is exceedingly rare in men, with fewer than ten well-documented cases published to date.1 The male breast typically contains little glandular tissue, which explains both the rarity of hamartoma and the striking visual contrast between fat and fibroglandular tissue when it does occur.
The triad of (1) oval or round morphology, (2) thin capsule and (3) heterogeneous internal fat-fibroglandular pattern appears in more than 90 % of hamartomas on mammography.2 Ultrasound mirrors this architecture, showing an encapsulated, parallel, heterogeneous, avascular mass. When all features are present-and no suspicious calcifications, angular margins or skin changes coexist-the BI-RADS lexicon allows a benign (category 2) assessment, obviating biopsy.3 Our patient fulfilled every criterion, and the long symptom duration without change further reinforced benignity.
Most solid male breast masses require tissue diagnosis because male breast cancer may appear deceptively benign; a classic hamartoma is an exception. Benign mimics include pseudoangiomatous stromal hyperplasia (PASH; circumscribed solid mass or focal asymmetry without internal fat), myofibroblastoma (well-circumscribed homogeneous solid mass in men, no fat), hemangioma (circumscribed mass with internal vascular channels/flow or phleboliths), and intraductal papilloma (retroareolar intraductal nodule with duct ectasia and Doppler flow). Other differentials in men comprise nodular gynaecomastia (ill-defined, flame-shaped subareolar proliferation, purely fibroglandular, non-encapsulated), lipoma (entirely fat-density with a thin capsule and homogeneous echogenicity), and carcinoma (irregular/spiculated margins, desmoplastic reaction, or suspicious microcalcifications/skin-nipple changes). Recognising the “breast-within-a-breast” sign and the mixed fat-fibroglandular composition is therefore crucial, as it supports a benign BI-RADS 2 assessment and may avert unnecessary biopsy when present.3
Although malignant transformation within a hamartoma is exceptionally rare, isolated reports justify continued surveillance.1 We recommend yearly clinical examination, reserving imaging for interval enlargement or new clinical findings-an approach aligned with published experience in both sexes.2

