











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Case Presentation
A 40-year-old woman presented with a sudden onset of severe headache. She denied focal neurological deficits or previous similar episodes. Her medical history was unremarkable, but she reported a family history of cerebral aneurysm. Non-contrast head CT showed no evidence of hemorrhage or infarction (not shown). Intracranial CT angiography (Fig. 1) revealed a small focal filling defect along the anterior wall of the proximal third of the basilar artery, characterized by a thin membrane protruding into the vascular lumen, consistent with a basilar artery web. No aneurysm, dissection, or significant stenosis was identified. The patient was managed conservatively with antiplatelet therapy and remains under clinical and imaging follow-up.
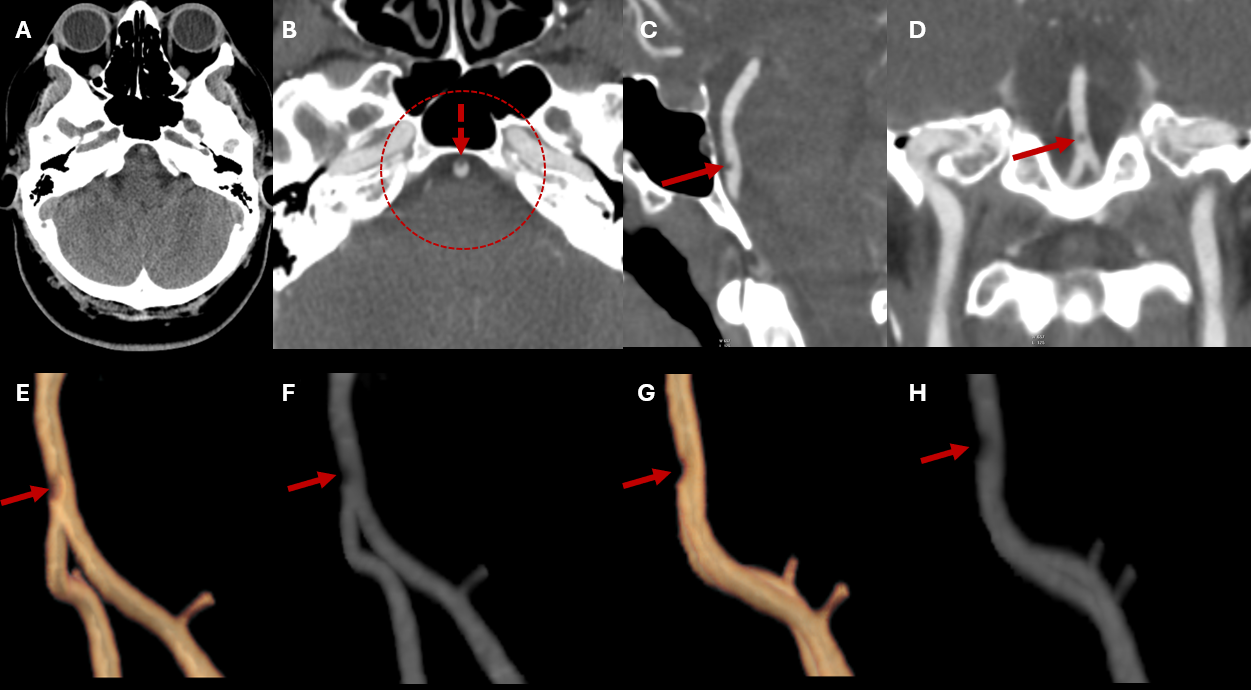
Figure 1: Non-contrast head CT (A) and CT angiography (B-H) of the posterior circulation. The non-contrast CT shows no hyperdense abnormalities. On CTA (B), a small focal intraluminal filling defect is seen along the anterior wall of the proximal basilar artery (arrow). Zoomed-in views in sagittal, coronal, and oblique reconstructions (C-H) better demonstrate this focal luminal defect, whose appearance is consistent with a thin membranous web.
Discussion
The basilar artery web (BAW) is a rare and likely under-recognized pathological intimal lesion of the posterior circulation. It is characterized by a thin, smooth, membranous projection extending into the arterial lumen. Histologically, it is considered part of the fibromuscular dysplasia (FMD) spectrum, representing focal intimal hyperplasia without evidence of atherosclerosis or inflammation. Although carotid webs are more extensively documented, this entity is increasingly reported as potential sources of ischemia in young or middle-aged individuals lacking conventional vascular risk factors.
From a pathophysiological perspective, the shelf-like intimal projection may disturb laminar flow, generating areas of stasis and turbulence that predispose to local thrombus formation or distal embolization.1,2,3In addition, the membrane may compromise perfusion of perforating branches, contributing to brainstem ischemia. Computational fluid dynamics studies support these mechanisms by demonstrating regions of low wall shear stress, recirculation flow patterns, and steep wall shear stress gradients adjacent to the web.4 These hemodynamic alterations may increase the likelihood of thrombosis or occlusion of perforating arteries. Some authors have also hypothesized that certain BAWs may represent variants within the spectrum of basilar artery fenestration-typically congenital and asymptomatic-but with potential clinical relevance when associated with ischemic events.5
Imaging plays a central role in diagnosis. On CT angiography (CTA) or digital subtraction angiography (DSA), a BAW typically appears as a smooth, small focal filling defect along the proximal/mid-basilar artery. Because our patient remained clinically stable, without focal neurological deficits or recurrent symptoms, no additional imaging studies-such as high-resolution MRI, digital subtraction angiography, or transcranial Doppler-were performed at that time. The CTA findings were considered sufficient to characterize the lesion and excluded immediate differential diagnoses, and further evaluation was reserved for follow-up should new symptoms arise. High-resolution black-blood MRI (HR-MRI) improves visualization of the membranous structure and aids in differentiating webs from thrombus, atherosclerotic plaque, or arterial dissection, in appropriate clinical scenario. Time-of-flight MRA (TOF-MRA) may demonstrate focal narrowing but is less sensitive for direct membrane depiction. In select anatomical investigations, intravascular angioscopy and histological analysis have confirmed layered vessel wall elements, supporting a congenital or developmental origin.
Although evidence remains scarce, current reports suggest that BAW management generally parallels carotid web treatment due to similar flow-related thromboembolic mechanisms. Most symptomatic patients have been successfully treated with antiplatelet therapy, including cases of brainstem infarction managed with aspirin alone1. Anticoagulation may be considered in the presence of recurrent embolic events or intraluminal thrombus, although supportive data for basilar lesions are limited. Endovascular approaches such as angioplasty or stenting have been described only in selected refractory cases, with no consensus favoring routine intervention. Given our patient’s stability and absence of ischemia, conservative management with single antiplatelet therapy and follow-up was deemed appropriate.
Conclusion
Basilar artery web is a rare but important vascular anomaly potentially associated with posterior circulation ischemia. It should be considered in patients presenting with cryptogenic neurological symptoms or headache, particularly when imaging shows intraluminal abnormalities of the basilar artery. Early recognition is crucial for appropriate management and to avoid misdiagnosis, especially in distinguishing BAW from thrombus, dissection, or anatomical variants.

