











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Case Presentation
A 39-year-old male, recreational jiu-jitsu practitioner, presented with right knee pain and functional limitation 15 days after a training injury. The trauma occurred during a defensive maneuver, when he sustained a combined varus and rotational force to the knee, followed by immediate pain, swelling, and inability to continue the activity. He denied previous injuries or comorbidities. The patient reported progressive difficulty with daily activities such as climbing stairs, walking long distances, and squatting, along with a subjective sensation of instability and “giving way” of the knee during ambulation. On examination, there was joint effusion, posterolateral tenderness, and flexion limited to 90° due to pain. The posterior drawer test was clearly positive, as were the external rotation (Dial) and varus stress tests, indicating posterior cruciate ligament (PCL) and posterolateral corner (PLC) involvement. Neurovascular status was preserved. Magnetic resonance imaging revealed complete ruptures of the PCL and lateral collateral ligament (LCL), partial tears of the popliteofibular ligament and popliteus tendon, with associated capsuloligamentous injury of the posterolateral complex, as well as an avulsion fracture of the fibular styloid (“arcuate sign”) (Figure 1). Surgical treatment was recommended due to the extent of injury, instability, and functional impairment. Patient consent for publication was obtained.
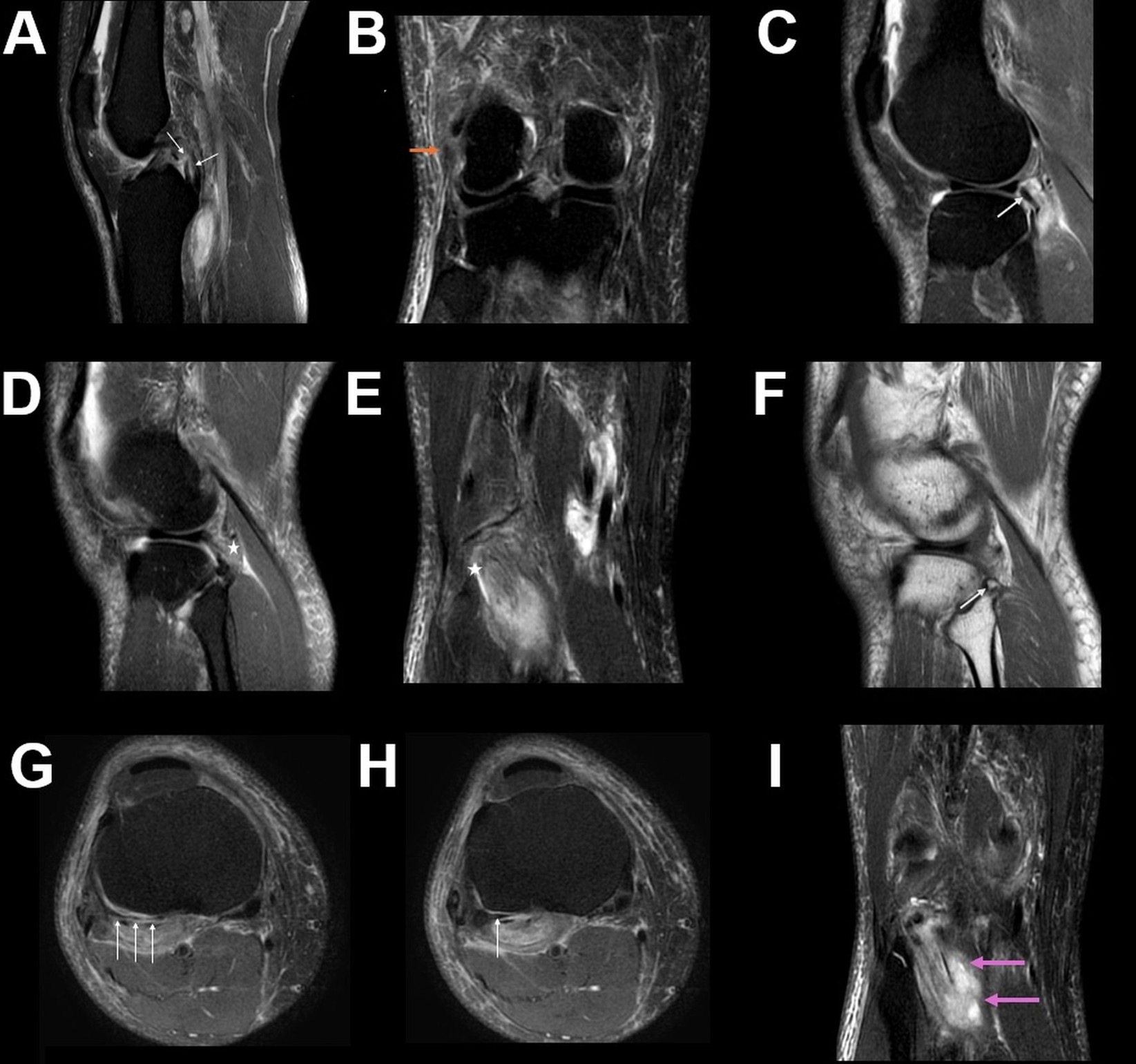
Figure 1: Magnetic resonance (MR) images using T2-weighted fat-suppressed (FAT SAT) and T1-weighted sequences demonstrating a multiligamentous posterolateral knee injury. (A) Sagittal T2 FAT SAT image showing complete rupture of the posterior cruciate ligament (white arrows). (B) Coronal T2 FAT SAT image showing rupture of the lateral collateral ligament (orange arrow). “(C) and (D) Sagittal T2-weighted fat-suppressed images and (E) coronal T2-weighted fat-suppressed image demonstrating the popliteus tendon (white arrow), with indistinct fiber delineation of the popliteofibular ligament consistent with rupture (asterisks).”. (F) Sagittal T1-weighted image demonstrating avulsion of the fibular head styloid process is also present (white arrowhead). (G and H) Axial T2-weighted fat-suppressed sequence demonstrates capsuloligamentous edema of the posterolateral complex (arcuate region) (white arrows). (I) Coronal T2 FAT SAT image showing injury at the myotendinous junction of the popliteus muscle (pink arrows).
Discussion
Multiligamentous knee injuries are uncommon but clinically significant, particularly when involving the posterior cruciate ligament (PCL) and the posterolateral corner (PLC). They frequently result from combined varus and rotational mechanisms, especially during sports activities such as martial arts.¹ Although the true incidence is likely underestimated, these injuries constitute an important cause of knee instability and functional impairment. The PLC rarely fails in isolation, and associations with PCL rupture are well documented, while concomitant injuries to the anterior cruciate ligament, menisci, or even neurovascular structures may also occur depending on the trauma mechanism.1,3
Magnetic resonance imaging (MRI) plays a central role in the evaluation of suspected PLC injuries. The main stabilizing structures of the PLC-namely the lateral collateral ligament (LCL), the biceps femoris tendon, and the popliteus tendon-are consistently the easiest to visualize and are crucial for assessing posterolateral stability.2,3 Their involvement strongly correlates with clinically significant instability patterns. In contrast, smaller components of the PLC may be variably seen, but their visualization is not essential to diagnose PLC injury.3
The terminology surrounding the so-called “arcuate ligament” remains controversial, as many authors question its definition as an independent structure.3 For this reason, and in line with contemporary radiologic descriptions, the finding in this case was interpreted as capsuloligamentous injury of the posterolateral complex rather than disruption of a discrete arcuate ligament.
Sports-related mechanisms are increasingly recognized as an important cause of multiligamentous injuries, and not all cases derive from high-energy trauma.1 Clinical diagnosis remains challenging, since the physical examination may be nonspecific, although the posterior drawer and Dial test offer valuable diagnostic clues.
Management depends on several factors, including the severity of the injury, time of diagnosis, and the patient’s functional demands. In general, posterior drawer displacement greater than 10 mm, persistent instability, or pain are indicators for surgical intervention, particularly in active patients who fail to improve with conservative measures. Surgical approaches continue to evolve, with anatomical reconstructions and arthroscopic-assisted techniques offering promising results, reduced morbidity, and improved functional outcomes.
Early recognition of combined PCL and PLC injuries is crucial to prevent chronic instability and degenerative changes. MRI, particularly with multiplanar protocols, remains the cornerstone for detecting subtle findings such as the arcuate sign. This case highlights the importance of correlating clinical examination with imaging to guide timely management and optimize outcomes.

