










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkActa Portuguesa de Nutrição
versão On-line ISSN 2183-5985
Acta Port Nutr no.15 Porto dez. 2018
https://doi.org/10.21011/apn.2018.1502
ARTIGO ORIGINAL
Body Mass Index and disordered eating behaviors: a cross-sectional study of a community sample participating in an obesity awareness campaign
Índice de Massa Corporal e Comportamentos Alimentares Problemáticos: Estudo Transversal de Amostra Comunitária Recolhida em Campanha de Sensibilização para a Obesidade
Sofia Ramalho1,2*; Ana Marinho2,3#; Ana Pinto-Bastos1,2#; Ana Vieira1,2#; Carina Magalhães1,2#; Cátia Silva1,2#; Susana Pedras1,2#; Silvia Pucci1,2#; Rosana Moysés2,4#; Tânia Rodrigues1,2#; Marta de Lourdes1,2#; Eva Conceição1#
1Escola de Psicologia da Universidade do Minho, Campus de Gualtar, 4710-057 Braga, Portugal
2Grupo de Estudo de Jovens Investigadores da Sociedade Portuguesa para o Estudo da Obesidade, Rua Freitas Gazul, n.º 34 - Loja 2,1350-149 Lisboa, Portugal
3Departamento de Ciências da Saúde Pública e Forenses e Educação Médica da Faculdade de Medicina da Universidade do Porto, Alameda Prof. Hernâni Monteiro, 4200-319 Porto, Portugal
4Departamento de Saúde Coletiva da Faculdade de Medicina da Universidade Federal do Amazonas, Av. Rodrigo Otávio, 6000 - Setor Norte do Campus, Manaus - AM, 69067-005, Brasil
#Estes autores contribuíram de forma equitativa para o estudo
Endereço para correspondência
ABSTRACT
Introduction: Several behavioral and lifestyle factors, including disordered eating behaviors, interact in the development and maintenance of overweight and obesity in adults.
Objectives: The present study aimed to describe the anthropometric, sociodemographic, and lifestyle characteristics, as well as the disordered eating behaviors of a community sample collected during an Obesity Awareness Campaign. Furthermore, the association between Body Mass Index, age, gender, food, beverages intake, and disordered eating behaviors is to be explored.
Methodology: This sample was composed of 109 participants (59% women, aged 39.7 ± 15.5 years; Body Mass Index 24.8 ± 3.6) who agreed to participate in an Obesity Awareness Campaign promoted in a shopping mall in the north of Portugal. Body Mass Index and disordered eating behaviors (uncontrolled eating, emotional eating, and cognitive restriction) were the main measures evaluated.
Results: Participants with obesity presented significantly more uncontrolled eating and emotional eating levels when compared to participants with overweight and normal Body Mass Index. No statistically significant differences were found between genders, age groups (18-28; 29-39; 40-50; 51-61; over 62 years) and disordered eating behaviors.
Conclusions: The results seem to indicate a positive link between disordered eating behaviors (uncontrolled and emotional eating) with the intake of unhealthy food/beverages, which can consequently lead to increased caloric intake and difficulties in weight management. The present findings alert clinicians to the importance of assessing disordered eating behaviors in individuals with obesity, providing useful information to customize clinical recommendations and intervention strategies, mainly in regard to the associations between food/beverage consumption and disordered eating behaviors.
Keywords
Body Mass Index, Disordered eating behaviors, Emotional eating, Obesity, Uncontrolled eating
RESUMO
Introdução: Múltiplos fatores comportamentais e de estilo de vida, incluindo comportamentos alimentares problemáticos, interagem no desenvolvimento e manutenção do excesso de peso e obesidade em adultos.
Objetivos: O presente estudo teve como objetivos descrever as principais características de uma amostra comunitária recolhida durante uma Campanha de Sensibilização para a Obesidade, ao nível de variáveis antropométricas, sociodemográficas, de estilo de vida, e de comportamentos alimentares problemáticos. Além disso, foram também exploradas as associações entre Índice de Massa Corporal, idade, género, alimentação, consumo de bebidas açucaradas e comportamentos alimentares problemáticos.
Metodologia: A amostra foi constituída por 109 indivíduos (59% mulheres, idade 39,7 ± 15,5 anos; Índice de Massa Corporal 24,8 ± 3,6) que aceitaram participar numa Campanha de Sensibilização para a Obesidade promovida num centro comercial no norte de Portugal. Índice de Massa Corporal e comportamentos alimentares problemáticos (comer de forma descontrolada, fome emocional e restrição cognitiva) foram as principais medidas avaliadas.
Resultados: Participantes com obesidade apresentaram pontuações mais elevadas nas subescalas de ingestão alimentar compulsiva e fome emocional, quando comparados a participantes com excesso de peso e Índice de Massa Corporal normal. Não foram encontradas diferenças estatisticamente significativas entre os géneros, grupos etários (18-28; 29-39; 40-50; 51-61; ≥62 anos) e comportamentos alimentares problemáticos.
Conclusões: Os resultados parecem sustentar a existência de uma associação positiva entre comportamentos alimentares problemáticos e a ingestão de alimentos/bebidas não saudáveis, que podem, consequentemente, levar a um aumento da ingestão calórica e a dificuldades no controle de peso. Os dados encontrados alertam os clínicos para a importância de avaliar comportamentos alimentares problemáticos em indivíduos com obesidade, fornecendo informações úteis para personalizar recomendações clínicas e estratégias de intervenção, principalmente no que diz respeito às associações entre ingestão alimentar (alimentos/bebidas) e comportamentos alimentares problemáticos.
Palavras-chave
Índice de Massa Corporal, Comportamentos alimentares problemáticos, Fome emocional, Obesidade, Ingestão alimentar compulsiva
INTRODUCTION
Obesity is defined by the World Health Organization (WHO) as a disease in which excess body fat can reach values capable of affecting health and quality of life in general (1). In Europe, about 30 to 70% of the adults are overweight and 10 to 30% are obese (2). In Portugal, 52.8% of adults with more than 18 years old have pre-obesity or obesity (3). Body Mass Index (BMI), in spite of its limitations related to the inability of discriminate different body compositions and accurately represent adipose tissue distribution (4, 5), is frequently used as an inexpensive and practical anthropometric indicator of nutritional status in adult community samples, enabling to identify adults with overweight or obesity (1, 6).
The causes of obesity are multi-faceted and several modifiable factors contribute and interact in the development and maintenance of overweight and obesity in adults. Particularly lifestyle factors as unhealthy diets, low physical activity levels, short sleep duration (1, 7, 8) and the presence of disordered eating behaviors such as dietary restraint, loss of control over eating and the tendency to overeat in the presence of emotional distress (9).
Moreover, the concomitance of disordered eating behaviors and obesity in adults seems to exacerbate physical and psychosocial impairments (10). For instance, disinhibition towards food consumption seems to be associated with higher BMI, unhealthy food choices and weight gain in adults (11–13). Furthermore, in a non-clinical sample, individuals with an eating behavior pattern characterized by uncontrolled eating and emotional eating above the median revealed the highest BMI values (14). When compared to men, women scored higher in cognitive dietary restraint and disinhibition towards food (11, 12).
In the context of this epidemic disease, awareness actions about obesity can be useful in promoting the adoption of healthy behaviors and in increasing health literacy, being this preconized as a valuable strategy for obesity prevention (15). This study examines data from a community sample collected during an obesity awareness campaign in the north of Portugal, the region with the highest prevalence of pre-obesity in Portugal (16).
OBJECTIVES
The aim of the present study is two-fold: 1) to describe the anthropometric, sociodemographic, lifestyle and disordered eating behaviors of a community sample collected in Braga (Portugal) during an obesity awareness campaign; 2) to further explore the association between BMI, age, gender, food, and beverages intake and disordered eating behaviors (uncontrolled eating, emotional eating, and cognitive restraint).
METHODOLOGY
Participants and Procedures
This is an observational, quantitative and cross-sectional study with a convenience sample. Both university ethics review board and the commercial space involved in the awareness campaign approved the study. Written informed consent was obtained from all the participants. One hundred and eighty-seven adults participating in the obesity awareness campaign activities aged between 18-80 years were invited to participate. Exclusion criteria were the presence of a mental disability and not being able to understand/read Portuguese. The data was collected over a single day (13 hours) during an obesity awareness campaign organized on the occasion of the “World Obesity Day” in October of 2017. The campaign activities included: 1) free health screenings with an assessment of weight, waist circumference, and blood pressure; 2) individual counseling with nutritionists; 3) film projections about obesity; and 4) dissemination of information about healthy lifestyle habits and obesity through flyers. After signing the informed consent, participants completed a 15-minute evaluation that included a set of self-report measures and an anthropometric/clinical assessment.
Measures
A semi-structured interview covering sleep patterns, sedentary habits (sitting time), and alcohol consumption was conducted, as well as a sociodemographic questionnaire addressing age, education, residence and marital, and professional status.
Anthropometric data: 1) weight was measured using a SECA flat scale (SECA model 899, SECA Corp., Hamburg, Germany, 2008); 2) Height was self-reported (in centimeters); 3) waist circumference was measured midway between the lowest ribs and the iliac crest; 4) blood pressure was measured in a seated position after the participant had rested for at least 5 minutes with a Haeger automatic blood pressure monitor (TM-ARM.002A model).
The frequency of food and beverages intake during the previous month was assessed through a food frequency questionnaire (FFQ), validated for the Portuguese population (17). A single-item was used to assess physical activity during the last week, “In the past week/past month, on how many days have you performed a total of 30 minutes or more of physical activity, enough to raise your breathing rate? (…)”(18). The Three-Factor Eating Questionnaire-Revised 21 (TFEQ-R21) was used to measure different aspects of disordered eating behavior. This questionnaire consists of 21 items that generate three subscales: cognitive restraint, emotional eating, and uncontrolled eating. Higher scores are indicative of greater cognitive restraint, uncontrolled, or emotional eating (19). Lastly, a single-item from the 36-item Short Form Health Survey (SF-36) was used to assess the general quality of life, “In general, would you say your health is: excellent, very good, good, fair, or poor?” (20).
Data Analysis
The statistical analysis was conducted with IBM SPSS Statistics 24.0 (SPSS Inc., Chicago, IL, 2016). To assess the socio-demographic, anthropometric, clinical and lifestyle characteristics of the sample, descriptive statistics, including means and frequencies, were conducted. To investigate associations among anthropometric, clinical, disordered eating behaviors and lifestyle characteristics, Pearson´s (r) and Spearman´s (rs) correlation coefficients were used. Spearman´s partial correlations were performed to control the influence of age and gender in the associations between disordered eating behaviors and food/beverages intake over the last month. Independent samples t-test (t) were used to assess between-gender differences with respect to the variables under study. Kruskal-Wallis test (χ2) was performed to test differences between BMI and age groups regarding eating behaviors and Mann-Whitney test (U), with Bonferroni corrections, employed to reduce the chances of Type I errors.
RESULTS
Of the 109 Caucasian participants in the awareness campaign – World Obesity Day, 41 % (n = 45) were men and 59 % (n = 64) were women. Most of the participants were married (36.7%), employed (52.3%) and had completed high school (35.8%).
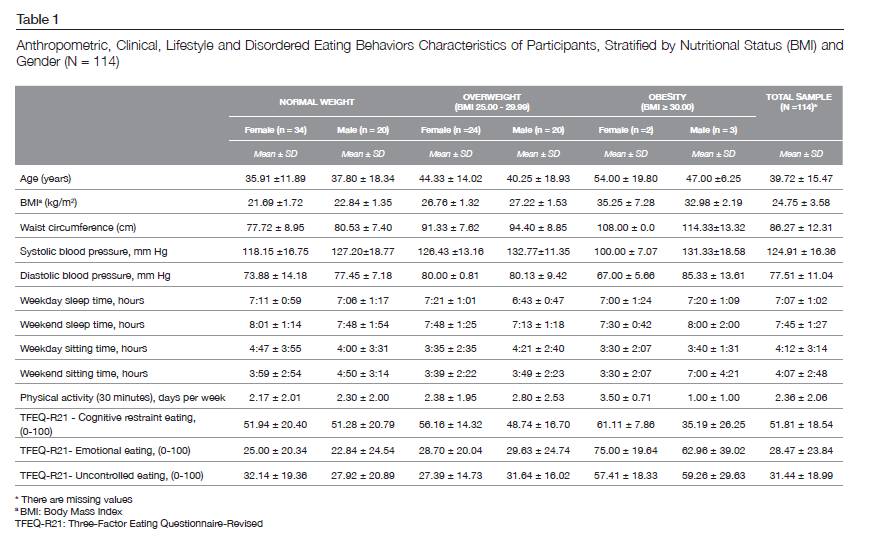
Regarding anthropometric indicators of nutritional status and according to the WHO BMI classification, 52.3% of participants had normal weight, 43.1% overweight and 4.6% obesity. Participants’ anthropometric, clinical, lifestyle characteristics and disordered eating behaviors, stratified by nutritional status (BMI) and genders, are described in Table 1.
Correlational analyses were performed to determine the associations between BMI, anthropometric, clinical and lifestyle variables. BMI was positively associated with waist circumference (r = 0.78; p < 0.001), age (rs = 0.28, p = 0.004), systolic (r = 0.24, p = 0.02) and diastolic blood pressure (rs = 0.28, p = 0.004). Positive significantly associations were also found between waist circumference, age (rs = 0.40, p < 0.001), systolic (r = 0.31, p = 0.003) and diastolic blood pressure (rs = 0.35, p < 0.001). Waist circumference and number of hours of sleep in a weekday were negatively correlated (rs = -0.28, p = 0.01). A higher number of hours of sleep in weekends were associated with lower BMI (rs = -0.20, p = 0.04).
Statistically significant differences were found between women and men regarding BMI (t (107) = 2.22, p = 0.02), waist circumference (t (87) = 2.19, p = 0.03), and systolic blood pressure (t (103) = 3.04, p = 0.003) with men reporting higher values in all variables. In this sample, the overall quality of life was mostly described as “good” (45%), 33% as “fair”, 16% as “very good”, 4% as “excellent” and 2% as “poor”. BMI was negatively associated with overall quality of life (rs = -0.25, p = 0.01).
Foods/beverages monthly intake and disordered eating behaviors
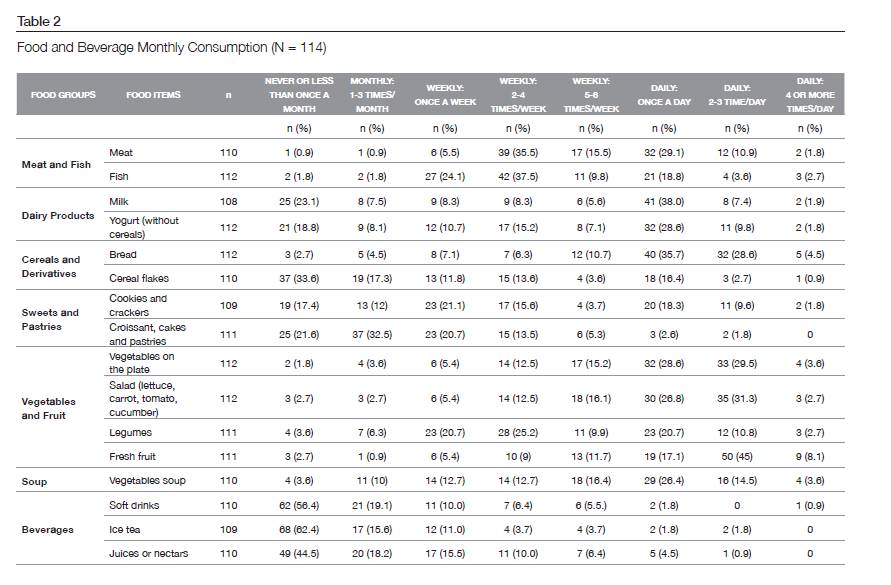
The frequency of consumption of foods and beverages from the previous month is described in Table 2. Additionally, correlation analysis between frequency of consumption of foods and beverages, anthropometric and lifestyle variables showed that systolic blood pressure was negatively associated with monthly consumption of yogurt (rs = -0.34, p < 0.001), vegetables on the plate (rs = -0.23, p = 0.02), and fresh fruit (rs = -0.22, p = 0.02). On turn, weekend sitting time was positively associated with monthly consumption of nectars/juices (rs = 0.23, p = 0.02) and meat (rs = 0.24, p = 0.02), as hours of sleep during weekdays with sweetened ice tea (rs = 0.21, p = 0.03).
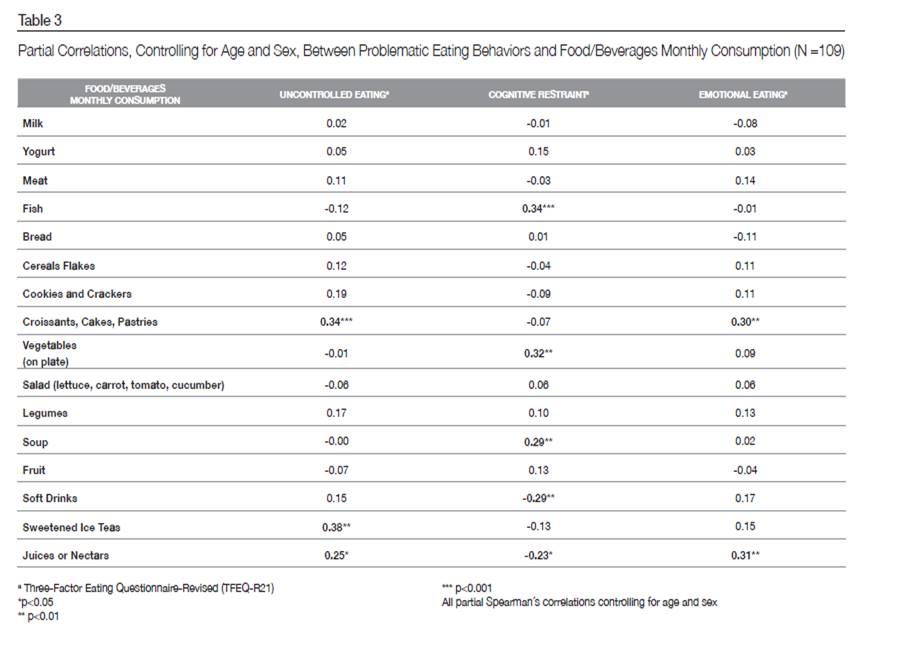
Table 3 presents partial correlations, controlling for age and gender, between disordered eating behaviors (uncontrolled eating, emotional eating, and cognitive restraint) and food/beverages intake over the last month. The results indicated that uncontrolled eating and emotional eating are significantly and positively correlated with higher monthly consumption of croissants, cakes, pastries, and juices/nectars. Moreover, emotional eating was also significantly and positively associated with more sweetened ice teas’ consumption. In turn, higher levels of eating restraint seemed to be related to a healthier dietary pattern, being positively correlated to the intake of fish, vegetables, and soup. In its turn, being significantly related to lower consumption of sweetened beverages, namely soft drinks and juices/nectars (Table 3).
Gender, Age, BMI and disordered eating behaviors
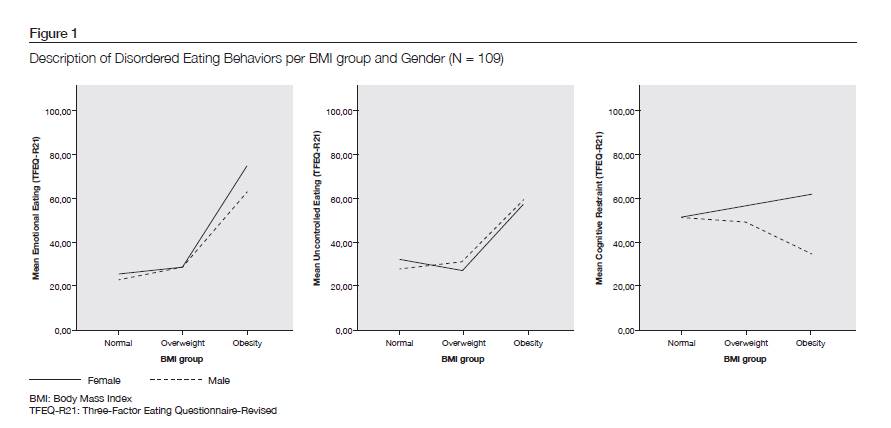
Figure 1 depicts the description of disordered eating behaviors (uncontrolled eating, emotional eating, and cognitive restraint) per BMI group and gender.
Statistically significant differences were found between BMI groups (normal weight, overweight, obesity), uncontrolled eating (χ2 (2) = 6.45, p = 0.04) and emotional eating (χ2 (2) = 8.87, p = 0.01). Participants with a BMI ≥ 30 (obesity) presented significantly more uncontrolled eating (Mean (SD) = 58.52 ± 22.89) when compared with participants with overweight BMI (U = 35.00, p = 0.008; Mean (SD) = 30.76 ± 17.84) and normal BMI (U = 48.50, p = 0.013; Mean (SD) = 30.73 ± 19.63). Similarly, participants with a BMI ≥ 30 presented significantly more emotional eating (Mean (SD) = 67.78 ± 30.02) when related with participants with overweight BMI (U = 33.50, p = 0.007; Mean (SD) = 29.14 ± 22.10) and normal BMI (U = 34.00, p = 0.004; Mean (SD) = 24.28 ± 21.62).
No statistically significant differences were found between genders, age groups (18-28, 29-39; 40-50; 51-61; over 62 years) and disordered eating behavior variables (uncontrolled eating, emotional eating, and cognitive restraint) (Figure 1).
DISCUSSION
The current study examined and characterized the associations between BMI groups (normal weight, overweight, and obesity), gender, age, lifestyle variables, monthly intake of foods/beverages and disordered eating behaviors in a community sample of adults.
The data suggest that adults with a BMI ≥ 30 (obesity) presented significantly more uncontrolled and emotional eating when compared with participants with overweight and normal weight. These findings are consistent with the existent literature (21, 22), although we did not find differences between overweight and normal weight BMI classification groups. These contradictory results seem to be in line with another Portuguese study that did not find an straight association between BMI classification, uncontrolled and emotional eating (23) possibly reflecting the BMI’s limitations as an obesity indicator. In fact, individuals with overweight seeking weight loss may present more disturbed eating behaviors when compared with non-seeking treatment overweight individuals. In the present study, the seeking treatment variable was not controlled, which might be a reasonable explanation for the confounding results (22).
No significant differences were found between BMI classification groups and cognitive restraint. Current literature is contradictory about this topic presenting conflicting results (24). On the one hand, some studies suggest an association between cognitive restraint and a higher weight (23, 25, 26), on the other there is some evidence showing that higher levels of cognitive restraint during a dietary intervention can produce greater weight loss (27).
Furthermore, no differences were found between gender and age groups regarding the disordered eating behaviors evaluated by TFEQ-R21, namely uncontrolled eating, emotional eating, and cognitive restraint. In spite of the current literature suggesting the existence of gender differences in problematic eating behaviors, mixed results were found. Some studies describe higher scores in cognitive restraint and emotional eating for women, whereas others did not find significant gender differences regarding uncontrolled eating levels (23, 25, 26). Nevertheless, it is likely that women and men vary in terms of the food groups that they seek (28).
Overall, participants reported a healthy dietary pattern, with a high consumption frequency of vegetables and fruit on a daily basis and a low consumption frequency of soft drinks. Additionally, the consumption of food items, such as yogurt, vegetables on the plate and fresh fruit was related to lower systolic blood pressure, as corroborated by literature (29). At last, diets rich in fruit, vegetables, and dairy products were related to healthier blood pressure (29).
The results seem to indicate a positive link between disordered eating behaviors (uncontrolled and emotional eating) with the intake of unhealthy food/beverages, which can consequently lead to increased caloric intake and difficulties in weight management. These findings are partially supported by other studies with TEFQ in the general population (30).
On the other side, and despite the fact that overall literature supports a causal relation between restraint eating and disinhibited eating patterns, in the present study restraint eating appears to be associated with healthier food choices (31). These contradictory findings can be enlightened by the role that restraint eating can play in individuals with divergent BMI status. Johnson et al. (2012) discuss that in obese population restraint eating can be an adaptive behavior associated with weight loss, whereas in normal weight population the presence of restraint eating can suggest overeating tendencies (32).
Regarding sleep patterns, no differences were found between BMI groups and sleep duration. Waist circumference was negatively related to the number of hours of sleep during the week, a finding supported by other studies (33). Furthermore, it was possible to find an extension of 38 minutes on the mean duration of sleeping time during the weekend, when compared to the duration of sleep during the week. This pattern seem to be associated with lower BMI. In fact, weekend sleep extension seems to have a biological protective effect in minimizing the consequences of sleep loss and, subsequently, protecting against obesity (34).
Study limitations included the use of self-reported rather than measured current height, the use of retrospective assessments of food/beverages consumption, sleep patterns and sitting time, and the small sample size in the BMI obesity group, precluding generalizations. On the other hand, our current findings examined both men and women and are novel in that they characterize the population whiling to engage in the obesity awareness campaign activities. Our sample was mainly normal weighted and we hypothesized that individuals with obesity would not participate in public activities related with obesity due to body-shame issues and stigmatization. Future studies should consider replicating this study with a larger sample size, exploring not only problematic eating behaviors and its associations with BMI and dietary patterns, but also adaptive eating behaviors such as intuitive eating. It would also be valuable to conduct more complex statistical analyzes, as cluster analysis, in order to identify the sociodemographic and psychosocial characteristics of the individuals at higher risk for overweight and obesity, tailoring awareness campaigns in accordance with the participants level of risk. Lastly, it would be important to investigate participants’ expectations and perceptions about participating in awareness campaigns and their impact on health literacy and eating behaviors.
CONCLUSIONS
The results of this study reinforces the link between BMI, dietary patterns, and disordered eating behaviors, highlighting the importance of assessing and intervening on disordered eating behaviors in the field of health promotion and obesity prevention.
ACKNOWLEDGEMENTS
This research was partially supported by Fundação para a Ciência e a Tecnologia/Foundation for Science and Technology through a European Union COMPETE program grant to Eva Conceição (IF/01219/2014) and doctoral scholarship (SFRH/BD/104182/2014) to Sofia Ramalho, Ana Pinto Bastos (SFRH/BD/104159/2014) and (SFRH / BD / 80468 / 2011) Cátia Silva.
We would like to thank the Portuguese Association for the Study of Obesity (Sociedade Portuguesa para o Estudo da Obesidade (SPEO)) for their active involvement and financial support in the implementation of this awareness campaign. And also thank to the Associação de Estudantes da Escola Superior de Enfermagem Calouste Gulbenkian for their support in data collection.
REFERENCES
- World Health Organization. Obesity: Preventing and Managing The Global Epidemic : report of a WHO consultation. Geneva; 2000. Available from: https://www.who.int/nutrition/publications/obesity/WHO_TRS_894/en/.
- World Health Organization. Obesity and overweight [Internet]. Geneva: World Health Organization; 2018 Fev [cited 2019 Jan 20]. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
- Instituto Nacional de Estatistica. Inquérito Nacional de Saúde 2014.Lisboa: Instituto Nacional de Estatística; 2016.
- Nevill AM, Stewart AD, Olds T, Holder R. Relationship between adiposity and body size reveals limitations of BMI. Am J Phys Anthropol. 2006 Jan;129(1):151–6.
- Kok P, Seidell JC, Meinders AE. The value and limitations of the body mass index (BMI) in the assessment of the health risks of overweight and obesity. Ned Tijdschr Geneeskd. 2004 Nov;148(48):2379–82.
- Bailey KV, Ferro-Luzzi A. Use of body mass index of adults in assessing individual and community nutritional status. Bull World Health Organ. 1995;73(5):673–80.
- Thorp A, Owen N, Neuhaus M, Dunstan DW. Sedentary behaviors and subsequent health outcomes in adults: A systematic review of longitudinal studies, 1996-2011. Am J Prev Med. 2011;41(2):207–15.
- Wu Y, Zhai L, Zhang D. Sleep duration and obesity among adults: a meta-analysis of prospective studies. Sleep Med. 2014;15(12):1456–62.
- Pinto-Bastos A, Ramalho S, Conceição E, Mitchell E. Disordered eating in Obesity. In: Ahmad SI, Imam SK, editors. Obesity: A Practical Guide. Switzerland: Springer International Publishing; 2015.
- Goldschmidt A, Aspen V, Sinton M, Tanofsky-Kraff M, Wilfley D. Disordered eating attitudes and behaviors in overweight youth. Obesity. 2008;16(2):257–64.
- Kruger R, De Bray JG, Beck KL, Conlon CA, Stonehouse W. Exploring the relationship between body composition and eating behavior using the three factor eating questionnaire (TFEQ) in young New Zealand women. Nutrients. 2016;8(7):386.
- Provencher V, Drapeau V, Tremblay A, Després JP, Lemieux S. Eating Behaviors and Indexes of Body Composition in Men and Women from the Québec Family Study. Obes Res. 2003;11(6):783–92.
- French SA, Epstein LH, Jeffery RW, Blundell JE, Wardle J. Eating behavior dimensions. Associations with energy intake and body weight. A review. Appetite. 2012;59(2):541–9.
- Löffler A, Luck T, Then FS, Sikorski C, Kovacs P, Böttcher Y, et al. Eating Behaviour in the General Population: An Analysis of the Factor Structure of the German Version of the Three-Factor-Eating-Questionnaire (TFEQ) and Its Association with the Body Mass Index. PLoS One. 2015;10(7):e0133977.
- Malik VS, Hu FB. Obesity Prevention. In: Prabhakaran D, Anand S, Gaziano TA, Mbanya JC, Wu Y, Nugent R, editors. Disease Control Priorities. Third Edition. Cardiovascular, Respiratory, and Related Disorders. World Bank Publications; 2017.
- Direção-Geral da Saúde. Programa Nacional para a Promoção da Alimentação Saudável; 2017. Available from: https://www.alimentacaosaudavel.dgs.pt/activeapp/wp-content/files_mf/1507564169PNPAS_DGS2017.pdf.
- Lopes C. Diet and myocardial infarction: a community-based case-control study [PhD thesis].[Porto]: University of Porto; 2000.
- Milton K, Bull FC, Bauman A. Reliability and validity testing of a single-item physical activity measure. Br J Sports Med. 2011;45(3):203–8.
- Duarte P. The Three-Factor Eating Questionnaire-R21: A Confirmatory Factor Analysis in a Portuguese sample [master’s thesis]. [Coimbra]: Faculdade de Psicologia e Ciências da Educação da Universidade de Coimbra; 2015.
- Macias C, Gold PB, Öngür D, Cohen BM, Panch T. Are Single-Item Global Ratings Useful for Assessing Health Status? J Clin Psychol Med Settings. 2015;22(4):251–64.
- Stapleton P, Mackay E. Feeding feelings: Is there a relationship between emotional eating and body mass index in adults? Int J Heal Caring. 2015;15(3):1–10.
- Boschi V, Iorio D, Margiotta N, D’Orsi P, Falconi C. The Three-Factor Eating Questionnaire in the Evaluation of Eating Behaviour in Subjects Seeking Participation in a Dietotherapy Programme. Ann Nutr Metab. 2001;45(2):72–7.
- Duarte P, Palmeira L, Pinto-Gouveia J. The Three-Factor Eating Questionnaire-R21: a confirmatory factor analysis in a Portuguese sample. Eat Weight Disord. Forthcoming 2018.
- Hays NP, Roberts SB. Aspects of Eating Behaviors “Disinhibition” and “Restraint” Are Related to Weight Gain and BMI in Women. Obesity. 2008;16(1):52–8.
- de Medeiros ACQ, Yamamoto ME, Pedrosa LFC, Hutz CS. The Brazilian version of the three-factor eating questionnaire-R21: psychometric evaluation and scoring pattern. Eat Weight Disord. 2017; 22(1):169–75.
- Anglé S, Engblom J, Eriksson T, Kautiainen S, Saha M-T, Lindfors P, et al. Three factor eating questionnaire-R18 as a measure of cognitive restraint, uncontrolled eating and emotional eating in a sample of young Finnish females. Int J Behav Nutr Phys Act. 2009;6(1):41. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2720907/.
- James BL, Loken E, Roe LS, Rolls BJ. The Weight-Related Eating Questionnaire offers a concise alternative to the Three-Factor Eating Questionnaire for measuring eating behaviors related to weight loss. Appetite. 2017;116:108–14.
- Burton P, J. Smit H, J. Lightowler H. The influence of restrained and external eating patterns on overeating. Appetite. 2007 Jul;49(1):191–7.
- Ndanuko RN, Tapsell LC, Charlton KE, Neale EP, Batterham MJ. Dietary Patterns and Blood Pressure in Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Adv Nutr. 2016;(1):76–89.
- Lauzon B, Romon M, Deschamps V, Lafay L, Borys J-M, Karlsson J, et al. The Three-Factor Eating Questionnaire-R18 is able to distinguish among different eating patterns in a general population. J Nutr. 2004;134(9):2372–80.
- Pervanidou P, Chrousos GP, Pervanidou P, Chrousos GP, Charmandari E, Kino T, et al. Metabolic consequences of stress during childhood and adolescence. Metabolism. 2012;61(5):611–9.
- Johnson F, Pratt M, Wardle J. Dietary restraint and self-regulation in eating behavior. Int J Obes. 2012;36:665–74.
- Sperry SD, Scully ID, Gramzow RH, Jorgensen RS. Sleep Duration and Waist Circumference in Adults: A Meta-Analysis. Sleep. 2015;38(8):1269–76.
- Im HJ, Baek SH, Chu MK, Yang KI, Kim WJ, Park SH, et al. Association Between Weekend Catch-up Sleep and Lower Body Mass: Population-Based Study. Sleep. 2017;40(10). Available from: https://academic.oup.com/sleep/article/40/7/zsx089/3836093.
Sofia Ramalho
Escola de Psicologia da Universidade do Minho,
Campus de Gualtar,
4710-057 Braga, Portugal
sofia.mm.ramalho@gmail.com
Recebido a 28 de setembro de 2018
Aceite a 28 de dezembro de 2018


{kind=link}
{kind=link}
{kind=link}
{kind=link}