











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
Individual lifestyles are a common factor influencing the onset of non- -communicable diseases, considered the leading cause of morbidity and mortality in developed societies (1). Children's lifestyle assessment is crucial for developing and implementing effective policies that prevent diseases related to eating habits and physical inactivity and, thus, ensure health in the future (2). Also, accurate and valid assessments are essential to quantify problems, monitor changes over time and identify high-risk groups (2). The first years of life, especially between 6 and 9, are an essential phase of growth at all levels, ideal for transmitting important knowledge and creating healthy habits that can last for a lifetime (3). The literature reports the benefits of physical activity (PA) in the physical, mental, cognitive, social and academic performance of children and young people (5-17 years old), associating a higher frequency of PA with a better life quality related to health (4, 5). A healthy diet is recommended to reduce the risk of developing non-communicable diseases (6). The relationship between adequate intake of fruit and vegetables (FV) and prevention of various non- -communicable diseases is well established (7). Short sleep duration in children is also associated with a significantly increased risk of obesity (8). Years of maternal education were positively associated with increased diet quality from 4 to 7 years (9). Children with more PA equipment at home spent less time on sedentary behaviours (10). In children, as far as our knowledge, there is no previous healthy lifestyle index including more than one dimension. Therefore, this study aimed to develop an index that associates children’s food habits and behaviours, PA and sleep duration, characterizing their lifestyles and their association with maternal sociodemographic characteristics and house physical environment.
METHODOLOGY
Participants
The present study was based on data from baseline and the 7-year follow-up of the population-based birth cohort Generation XXI (11). This cohort included 8647 newborns at baseline that were recruited from the five public maternity hospitals in the metropolitan area of Porto between 2005 and 2006 (91.4% of invited mothers). The Generation XXI project is in line with the Declaration of Helsinki and was approved by the Ethics Committee of the Hospital de São João/University of Porto Medical School and by the Portuguese Authority of Data Protection. For the final sample, we considered all children with complete information on the variables of interest and excluded children with diseases that might influence food intake (celiac disease, allergy, and food intolerance) and children with congenital malformations that might affect feeding (n=24), achieving a final sample of 4336 children.
Data Collection
Children’s diet was collected through a previously calibrated 38-item food frequency questionnaire (FFQ) (12), assessing usual food consumption in the previous 6 months. The main caregivers were also asked about their perception regarding certain children's eating behaviours, such as if the child ‘do not eat enough’, ‘eat very slowly’ and/or ‘eat exaggerated amounts’. Children’s PA was characterized by the following activities: spending one daily hour or more in active play (running, cycling, playing ball), the practice of any scheduled and regular out-of-school PA and spending more than two daily hours in sedentary activities (reading, painting, studying, watching television and playing games on the computer or console), during the week or at the weekend. Duration of sleep was calculated as the difference between bedtime and wake-up time and bedtime.
Maternal working status was divided into two groups: 'paid situations' (full-time employee, employed part-time, employed less than part-time or retired/pre-retired) and 'unpaid situations' (familiar worker unpaid, unemployed, student, domestic or another situation). Household income was grouped as '≤1000 €', '1001-1500 €' and ‘>1500€’. The number of rooms was categorized as ‘1 to 3 rooms’, ‘4 rooms’ or ‘5 to 12 rooms’. Having access to the garden, to the internet, and a bicycle at 7 years of age was categorized as ‘yes’ or ‘no’.
The Healthy Lifestyle Index
For the current sample, the Cronbach alpha coefficient was obtained for the Healthy Lifestyle Index to assess its internal consistency. Initially, the Healthy Lifestyle Index included four domains (frequency of food consumption, eating behaviours, PA and sleep) and presented a Cronbach alpha value of 0.44. After excluding the questions of the domains 'eating behaviour' and 'sleep', the Cronbach alpha value increased to a maximum value of 0.52 and was considered the final index. Cronbach’s alpha is a method for assessing the instrument reliability by comparing the degree of common variance among the items of an instrument against the overall variance (13).
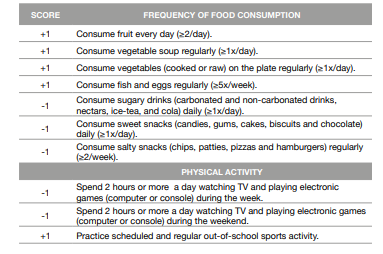
The construction of the final healthy lifestyle index was based on two domains: frequency of food consumption and PA (including sedentary behaviours) (Table 1). Behaviours considered healthier were scored 1 point, while others considered less healthy scored -1 point (Table 1). The final points were summed to obtain the final score of the developed index, ranging from -5 to 10 points, with higher scores reflecting a healthier lifestyle.
Statistical Analysis
Comparisons of continuous variables were performed using the Student's t-test and were summarized by means and SD. Categorical variables were described as frequencies and compared using the Chi-square test.
The associations between the sociodemographic characteristics and the physical environment of the house and the healthy lifestyle index at 7 years were evaluated through linear regression models - regression coefficients and respective 95% confidence intervals [β, 95%CI]. A step-by-step approach was used: predefined blocks of variables were fitted separately, each block mutually adjusted, and introduced cumulatively into the analysis, with a fixed order. Model 1 was adjusted for maternal age and education at delivery time and the child’s sex. Model 2 included maternal age, working status, child sex, and monthly household income. Model 3 included all variables of model 1 plus the number of rooms, garden, terrace, internet, bicycle, and computer.
RESULTS
Table 2 shows that mothers included in this sample were slightly older and more educated than those drawn from the larger cohort. Children in this sample practiced significantly more out-of-school PA (56.0%) than those in the remaining cohort (44.3%).
Table 2 Comparison between characteristics of eligible participants and the remaining cohort
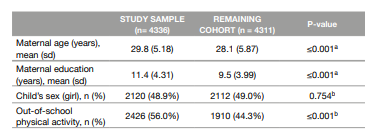
aStudent's t-test
bChi-Square test
SD:Standard deviation
Table 3 presents that most children (64%) consume five or more portions of ‘Fruits, vegetables and soup’ daily and ‘Fish and eggs’ at least 5 times per week. Almost half of the children (46%) consume ‘Sweets’ and ‘Soft drinks’ daily, and 27% consume ‘Salty snacks’ at least 2 to 4 times per week. Most children practice out-of-school scheduled and regular PA (56%). Only 15.6% of the children spend 2 hours or more a day in screen time during the week. However, this percentage increases to 69.9% during the weekend. The lifestyle index of children at 7 years had a mean score of 3.6 points (SD=2.8).
Table 3 Food intake and physical activity habits of children at 7 years of age
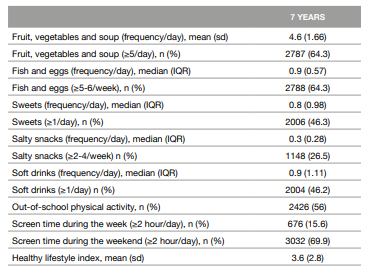
IQR: Interquartile range
SD: Standard deviation
In Table 4, it was described that higher maternal age and education was associated with a higher healthy lifestyle index score. Model 2 shows that children whose mothers have unpaid jobs have an inverse association with the index score compared to children whose mothers have paid work. Similarly, the higher the total household monthly income, the higher the index score. Also, in model 3, having access to the garden, internet, a bicycle, and living in a house with 5 or more rooms were significantly associated with a higher lifestyle index score.
Table 4 Association between sociodemographic factors, physical environment of the house and children’s BMI and adherence to a healthy lifestyle at 7 years old
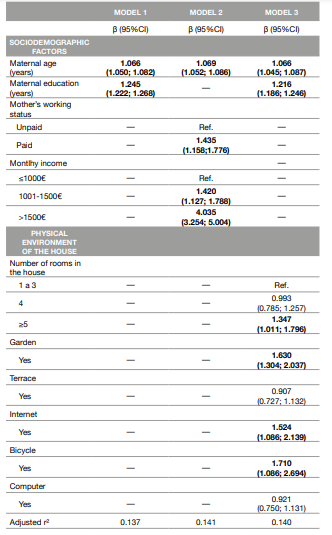
Model 1 was adjusted for maternal age and education at delivery time and the child’s sex.
Model 2 was adjusted for maternal age, working status, child sex, and monthly household income.
Model 3 included all variables of model 1 plus the number of rooms, garden, terrace, internet, bicycle, and computer.
DISCUSSION OF THE RESULTS
In the present study, the average lifestyle index score for children at 7 years old was 3.6 points on a scale ranging from -5 to 10. In a previous study exploring the association between PA status and several lifestyle characteristics in children and youth, participants classified as having inadequate levels of PA reported poorer eating habits, more screen time, and less sleep time. These children presented a worse lifestyle profile compared to those with adequate levels of PA (14). Thus, in the present study, the low score on the lifestyle index reflects unhealthy eating habits and low levels of PA in children of 7 years. Most children in this study fulfilled the WHO recommendations for daily consumption of at least 400 g of FV (5 or more portions per day). However, almost half of the children consume sweets and soft drinks daily, which does not fulfil the recommendations of a healthy eating pattern that should include limited consumption of ultra-processed foods, saturated and trans fats, added sugars and salt (15). In this study, most children practice scheduled and regular PA out-of-school. It is also reported that increasing PA during school hours is associated with children’s better physical, psychological, and social health (16). In the present study, the higher the level of the mother’s education at the time of the children’s birth, the better the children’s lifestyle at 7 years of age. A previous study (9) described that higher maternal education is related to increased children’s diet quality from 4 to 7 years of age, supporting our results. Another study concluded that children whose mothers had a lower level of education consumed less healthy foods (17). Children with more PA equipment have been found to spend less time on sedentary behaviours (18), and the lack of gardens was identified as a barrier to the practice of PA and active play (10, 19). These data support the positive association, verified in this study, between having access to a garden and a bicycle and having a better lifestyle index score. Besides that, as seen in this study, a better socioeconomic environment increases the Healthy Lifestyle Index score, which supports that the index has criterion validity.
One of the main strengths of this study is to focus on developing an instrument that identifies, in an early phase, less healthy lifestyles that could lead to non-communicable diseases. In that way, it can be used as a rapid diagnostic tool in schools, at a population level, by public health doctors, which allows the development of more sustainable and effective interventions that can correct those less healthy lifestyles. It might also be used in the clinical setting by nutritionists or general practitioners. Besides this, the study has a population basis allowing a greater scope and detail of the information.
Most of the information was obtained through the main caregiver report, which can lead to a misinterpretation of the questions asked (bias of social desirability). However, in the case of the FFQ used, it was previously calibrated and validated (12), and no relevant changes were expected. Additionally, despite the size of the cohort and its scope, children included in the cohort were recruited only in public hospitals. Assuming that the costs associated with childbirth in a private hospital are higher than in a public one, data available for this study may exclude children from higher economic class families. Thus, there may be some selection bias, although the number of children born in private hospitals was relatively low at the time of recruitment. Finally, we only used data from a single assessment, namely at 7 years of age and not at various time points, as part of a possible longitudinal study. In this way, it may limit the scope of the study to school-age children in general. In addition, assessing children at a younger age (preschool age) may be important.
CONCLUSIONS
The final healthy lifestyle index developed is a short instrument based on the frequency of food consumption and PA practice that was able to identify the low level of a healthy lifestyle in school-aged children. This instrument can be applied in future intervention studies and in clinical settings for a quick lifestyle assessment. Overall, children living in a house with access to a garden, internet, and bicycle and whose mothers were older and more educated had a healthier lifestyle.
FINANCIAL SUPPORT
Generation XXI was funded by the Health Operational Programme - Saúde XXI, Community Support Framework III and the Regional Department of Ministry of Health. This study was supported by the Portuguese Foundation for Science and Technology (FCT), under the Epidemiology Research Unit of the Institute of Public Health of the University of Porto (UIDB/04750/2020) and the Laboratory for Integrative and Translational Research in Population Health of the University of Porto (LA/P/0064/2020), and DOI identifiers https://doi.org/10.54499/UIDB/04750/2020 and https://doi. org/10.54499/LA/P/0064/2020. MPC benefited from an FCT individual doctoral grant (2020.08314.BD) [https://doi.org/10.54499/2020.08314.BD] and SV is supported by national funds through FCT, under the programme of ‘Stimulus of Scientific Employment -Individual Support’ within the contract 10.54499/2021.01096.CEECIND/CP1686/ CT0001 [https://doi.org/ 10.54499/2021.01096.CEECIND/CP1686/CT0001]. FCT had no role in the design, analysis or writing of this article.
ACKNOWLEDGMENTS
The authors gratefully acknowledge the families enrolled in Generation XXI for their kindness, all members of the research team for their enthusiasm and perseverance and the participating hospitals and their staff for their help and support.
AUTHORS’ CONTRIBUTIONS
BF: Responsible for the literature review, statistical analysis and interpretation, and writing the original draft preparation; MPC: Statistical analysis and interpretation, writing review and editing; SV: Study conceptualization, design, supervision and final approval. All authors read and provided critical feedback on the manuscript before the approval.

