











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
An increase in life expectancy was observed in human immunodeficiency virus (HIV) infection due to antiretroviral therapy (ARTc) (1, 2). However, the increase in underlying comorbidities, including cardiovascular disease (CVD), contributes to a high cardiovascular risk (CVR) showed to be 1.5 to 2 times higher, compared to non-infected patient (3-7). Adding, 90% of People living with human immunodeficiency virus (PLWHIV) aged 50 years or higher present at least one associated comorbidity and a modelling study suggests that in 2030, more than half of this group will have CVD (8-10). In addressing lifestyle as a prevention of comorbidities, moderate physical activity (PA) is recommended to decrease chronic inflammation, improving the individual’s metabolic health and survival (11,12). Adequate diet is another essential factor to prevent the onset of these complications, as well as contributing to a correct nutritional status (13). European guidelines show that dietary recommendations for PLWHIV are similar to the Mediterranean diet (MD) pattern, which reduces the risk of coronary disease, as proposed by Ancel Keys (14, 15). However, it has been shown that PLWHIV have a higher intake of total and saturated fat and cholesterol, when compared with uninfected people (16). This pattern, combined with a refined carbohydrate-rich diet, is associated with reduced nutritional quality (17).
OBJECTIVES
The purpose of this study is to assess the evolution of nutritional status, CVR and MD adherence and current PA level in a cohort with a mean follow-up of 5 years.
METHODOLOGY
This is a follow-up study from a cohort previously evaluated (18). Patients who maintained regular follow-up and agreed to participate in the reassessment were eligible for participation, resulting in 26% of the previously assessed. Due to the small sample size obtained, the odds of bias selection is high. Pregnant women, patients hospitalized in the last month or those who, after evaluation required hospitalization, were excluded. This study was conducted during a 6-month period. Data on systolic and diastolic blood pressure, lipid profile and glucose were assessed through the clinical process, as previously described (19). Data on diabetes, hypertension and smoking habits were obtained through personal interviews and the first two were confirmed by the clinical file, as previously described (19). Data on incident cardiovascular events and HIV infection was collected through the 5-year follow-up. All patients signed and the local Ethic Health Committee approved this study protocol. Data on weight and fat mass (FM) was obtained using a single-tetrapolar bioimpedance scale (Omron Body Composition Monitor BF511) (20, 21). FM was classified according to Gallagher and collaborators classification (22). Body mass index (BMI) was obtained taking into account the classification of the World Health Organization (23). Increased waist circumference (WC) was considered when the female sex had a WC≥80 cm and the male sex had a WC≥94 cm (24). Presence of metabolic syndrome (MS) was assessed based on Alberti and collaborators criteria (24). The presence of lipodystrophy was classified as previously (25, 26). A food frequency questionnaire and the MedDietScore were applied to assess food intake and adherence to the MD (baseline and 5th year) (27, 28). The long version of International Physical Activity Questionnaire - IPAQ was applied to assess the level of PA in the study population (5th year) (29). The CVR was assessed through DAD Risk Equation, developed specifically for PLWHIV (30). The data were analyzed both analytically and graphically using simple and comparative exploratory methods, including whisker plots, bar graphs, histograms, scatter diagrams, and calculations of minimum, maximum, mean, standard deviation, asymmetry coefficient, median, and quartiles, in relation to the variables and objectives presented in the study. Categorical variables were expressed as absolute number (percentage) and metric variables as mean ± standard deviation (minimum-maximum), when there was no significant asymmetry. The inferential analysis was based on the chi-square test for independent or homogeneous hypotheses involving the crossing of two categorical variables. To test the conditions of application of the Student T-test and one-way ANOVA and to compare mean values the normality tests were applied, Kolmogorof, with Lilliefors correction for n≥50, or Shapiro Wilks for n<50. Levene's equality of variance test was applied with a significance level of 5%. Bonferroni correction was applied to adjust multiple comparisons. In the event that the variables did not respect a normal distribution or violate the test applicability principles, nonparametric alternatives were used. For this study a significance level of 5% was used. All data were statistically analyzed using SPSS® software (IBM, version 26).
RESULTS
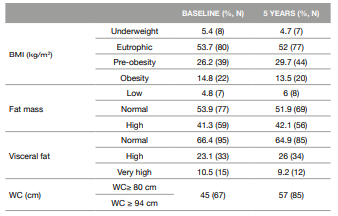
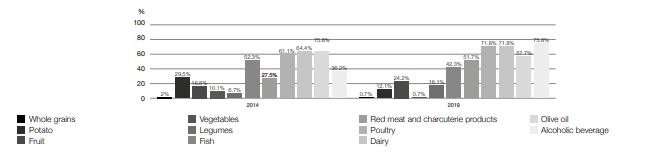
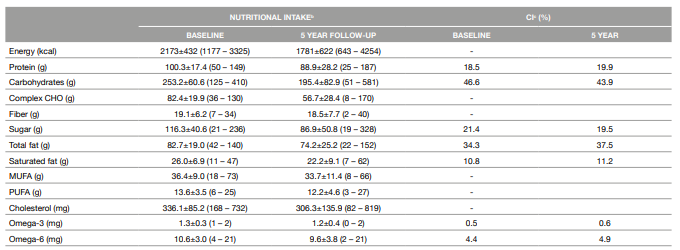
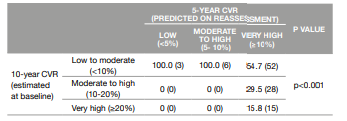
Patients who were submitted to a new nutritional evaluation (n=149) were mostly male Caucasian (61.7%; n = 92; 91.9%; n = 137, respectively) with a mean age of 52.0±9.3 years (Table 1). Regarding the occurrence of CVD there were cases of stroke (n=2), ischemic heart disease (n=2) and acute myocardial infarction (n=2). Patients were infected with HIV for 17.9±6.9 years, and more than half were under ARTc with mean exposure time of 15.8±6.6 years. There was a significant association between CVD and hypertension (p=0.018). Average BMI was 24.8±5.2 kg/m2, WC in female patients was 86.1±13.7 cm and in male patients was 95.2±13.8 cm. Compared with baseline there was a percentual increase in the pre-obesity category and increased WC prevalence (Table 2). Most patients did not present lipodystrophy (71.4%; n=95). The average score of MD adherence was 28.9±5.2 points, higher compared to baseline (27.9±5.7 points; p=0.026). There was an increase in the intake of fruit, fish, red meat and charcuterie products, poultry, dairy and alcoholic beverages (Figure 1). Adherence to whole grains, vegetables, potatoes, legumes, fruit and fish recommendations was less than 50%. The intake of fruit, dairy, fish and poultry did not show significant differences from baseline (p>0.05). There was no significant correlation between adherence to MD and anthropometric parameters. Patients had an average caloric intake (CI) of 1781±622 kilocalories (Kcal) (Table 3). During follow-up period there was a significant increase in protein (p<0.001), total (p=0.014) and saturated fat (p=0.002) intake. Individuals with hypertension presented a tendency to a reduction in cholesterol intake compared with baseline (p=0.054). The presence of dyslipidemia showed a significant positive association with CI (p=0.013) and total (p=0.012), saturated (p=0.012) and monounsaturated fat (p=0.02). Higher adherence to MD was positively correlated with a higher fiber intake (r=0.384; p<0.001). Regarding PA, more than half of the sample had a moderate level of PA (77.6%; n=111). Participants presented a mean daily sitting time of 244.4±173.9 minutes (about 4 hours/ day). There was no significant correlation between sitting time and anthropometric parameters or between sitting time and the PA level. The c-HDL showed an inverse correlation with sitting time (r=-0.252; p=0.004). The triglyceride levels also showed an inverse correlation with PA level (r=-0.183; p=0.033). Regarding CVR, when the baseline predictions were compared with 5 years, more than half of patients was at a very high CVR although the baseline estimation predicted a moderate to high risk (p<0.001) (Table 4). Correlations were found between the current CVR and weight (r=0.274; p=0.006), BMI (r=0.246; p=0.014), visceral fat (r=0.463; p<0.001) and WC (r=0.391; p<0.001). There was an association between 5-year CVR and MS (p=0.001).
There was no association between 5-year CVR and PA and MD (p>0.05). Through logistic regression it was demonstrated that hypertension was a significant predictor of the onset of CVD (OR 0.067; p=0.029; 95% CI, 0.006-0.755).
Table 1 Global characterization, biochemical data and characterization of HIV infection
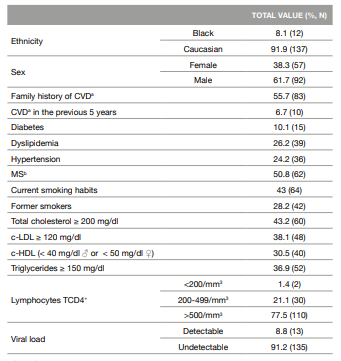
aCVD: Cardiovascular disease
bMS: Metabolic syndrome
DISCUSSION OF THE RESULTS
This study depicts the longitudinal nutritional status and documents the adherence to MD and PA of PLWHIV, scarcely characterized. Overweight is highly associated with a significant increased risk of developing CVD (31), underlining weight control as a parameter to be taken into account. In this group, 29.7% were overweight, a lower percentage than reported by Nalluga and collaborators (31). An increased WC as shown to be one of the factors that could be associated with an increased risk of CVD (32). Our study revealed a 10% growth in increased WC compared to baseline, higher than previously reported (33). Adherence to the MD showed an average score of 28.9±5.2 points, higher than baseline and previous reports (18, 34). Given that this is a longitudinal study, this group of patients may have increased their adherence due to a higher awareness in the first evaluation. Since the 1960s, adherence to MD pattern has been decreasing, with the exponential growth of the food industry and consequent emphasis on the Western Diet (17). Despite the increase adherence to MD compared with baseline, some groups showed an adherence of less than 50% (whole grains, potatoes, fruit, vegetables and legumes) suggesting an agreement with the Western pattern. The current average CI was 1781±622 Kcal/day, a lower value than demonstrated at baseline and by Hendricks and colleagues (35). This study also revealed that hypertension is a predictor of CVD as recognized by other studies (36, 37). Regarding dyslipidemia and fat intake, a significant positive association was found with total, saturated and monounsaturated fat. These results are in agreement with other studies, where saturated fat intake is a risk factor for the development of this comorbidity and monounsaturated and polyunsaturated fat are protective (38). Also, the significant positive association between dyslipidemia and CI is confirmed by a study of Nouri and colleagues, where the group with the higher ingestion of ultra-processed foods (3091.63±1275.98 kcal) had a higher lipid profile (39). More than half of the sample presented a moderate level of PA, in line with a systematic review where 50.7% reached the guidelines that recommend the practice of moderate PA (40). Since this group was aware of its CVR, it might have been one possible reason to explain this behavior (41). Patients spent a mean of four hours a day in sedentary behavior, a lower value than previously reported (42). The c-HDL showed an inverse correlation with sedentary behavior and triglycerides levels showed an inverse correlation with the PA level. The practice of PA in PLWHIV promotes a reduction in metabolic and CVR factors, improving quality of life (42). Regarding CVR, there was a severe deterioration in most of the individuals. This may be due to the tool calibration, with the addition of TCD4+ lymphocyte count parameter and the elimination of ART exposure (30, 43). Positive correlations were found between CVR and some anthropometric parameters, showing agreement with a recent study, that found an increase in CVR and also in WC and BMI (44). Current CVR and MD had no association. However, studies demonstrated that higher adherence to MD can trigger significant changes in the metabolome, directly related to cardiovascular and metabolic health (45). The disagreement between our results and Li study may be due to the small sample evaluated and to the different tool used to assess adherence to MD. Also, CVR and PA had no association, contrary to what has been shown in a study where moderate to vigorous PA is associated with a better cardiovascular health (46). However, 73.8% of this sample who was at very high CVR showed a moderate PA level, probably due to a recognition of their health and consequent change in behavior to a better health. This study has some limitations. The food frequency questionnaire used in this study refers to last year’s food consumption and requires memory for its complete filling. Also, overweight and obese patients tend to lack precision in measuring self-reported energy consumption (47). Regarding IPAQ, it has been shown that overestimation of the questionnaire’s self-completion in PLWHIV may occur (42). Furthermore, there is a wide variety of tools to assess adherence to PA and it is essential to reach a consensus about its use in PLWHIV (45).
CONCLUSIONS
Due to the comorbidities present in PLWHIV and verified in this group, acting on the modifiable risk factors becomes one of the most important aspects to reduce or prevent their appearance. Although it appears that they are already sensitized to some changes in lifestyle, there are still categories of MD that show low adherence. Therefore, it is essential to reinforce adherence to this dietary pattern and PA.

