











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
According to the Brazilian Institute of Geography and Statistics (1), by 2060 Brazil will have 25.49% of its population composed by elderly people.
There is a lack of programs and public policies that guarantee the preservation of autonomy and assistance to the elderly, who often have some dependence degree (2). When family members or guardians are unable to provide care, this role is taken on by long term care institutions, which take in these individuals and provide support for their basic daily needs (3).
Morbidities from this process, associated to chronic diseases and other factors can determine exposure to pressure injuries (PI), as well as slowing down their healing (4).
PI have a multifactorial etiology, and its development can be more significant in institutionalized older adults with compromised nutritional status (5, 6). In addition to worsening the quality of life, the PI affect the care dynamics and act as a quality marker of services provided in institutions, becoming a costly problem not only for Long Term Care (LTC), but also for public organizations and health services (7, 8).
OBJECTIVES
To assess the association between the occurrence of PI and nutritional status in the elderly.
METHODOLOGY
This was a retrospective observational cohort study and secondary data. The sample was by convenience and composed by all elderly who had come in six private LCT, in the last six months (Canoas and Porto Alegre cities, Rio Grande do Sul state, Brazil).
The study included older adults aged 60 or older, with at least 6 months' stay in the LCT and who signed the Informed Consent Form (ICF). In the case of older adults unable to understand and/or sign the ICF (mental or cognitive disabilities and/or psychological alterations), the document was signed by the legal guardian or by the institution coordinator, when the latter had a guardianship or a signed contractual document authorizing them to provide information for the study. Older adults who already had PI when they were admitted to the institutions were excluded. In cases where the elderly person, their legal guardian or the institution coordinator did not agree to sign the ICF, the participant was also excluded from the study.
Clinical, nutritional and sociodemographic data was collected from the elderly's medical records.
Weight and height measurement techniques were carried out in accordance with the procedure defined by the Brazilian Ministry of Health (8). Body Mass Index (BMI) was calculated using the Quetelet Index (weight/height2) (9) and assessed according to the Pan American Health Organization classification (10). Mini Nutritional Assessment (MNA) was also used to complement the nutritional diagnosis. In bedridden patients, weight and height were estimated by knee height (11), using the measurements proposed by Chumlea et al. (12), without using the subscapular skin fold and the technique used was that proposed by the International Society for Anthropometric International Society for the Advancement of Kinanthropometry (13).
PI presence was identified by means of a physical examination carried out by the LCT nurse and, in order to assess the PI stage, proposed classification of European Pressure Ulcer Advisory Panel (EPUAP), National Pressure Injury Advisory Panel (NPIAP) e Pan Pacific Pressure Injury Alliance (PPPIA) (14).
Quantitative variables were described by mean and standard deviation or mean and interquartile range. Categorical variables were described by absolute and relative frequencies. Student's t-test or Analysis of Variance (ANOVA) was used to compare means, along with Tukey's test. In the event of asymmetry, the Mann-Whitney and Kruskal-Wallis tests were used. The chi-square or Fisher's exact tests were used to compare proportions. In the event of statistical significance in the polytomous variables, the adjusted residuals were analyzed to locate the differences. Poisson regression multivariate analysis was used to control confounding factors. The criterion for entering the variable in the multivariate model was to have a p-value < 0.20 in the bivariate analysis and the criterion used to keep it in the final model was to have a p-value < 0.10.
Data were analyzed using the SPSS program version 27.0 (15) and the significance level was 5% (p≤0.05). This study was approved by Ethics Committee for Research of UNISINOS (protocol number 6.003.88), UNISINOS - University of Vale do Rio dos Sinos, Rio Grande do Sul state, Brazil.
RESULTS
Sample was composed by 178 older adults, with a mean age of 86 years (SD ± 8.8) and 135 (75.8%) female. White people represented 92.1% of the sample (Table 1).
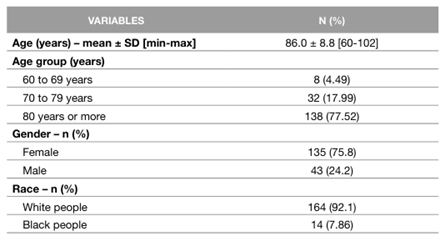
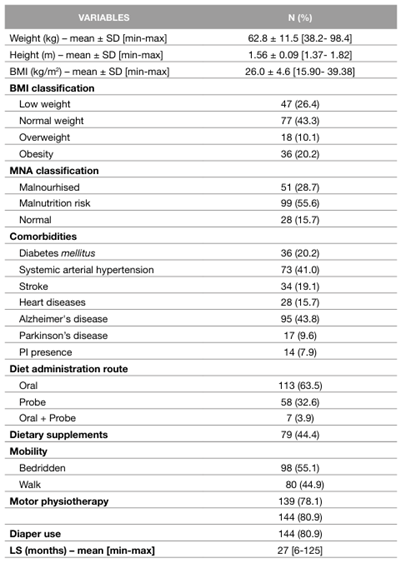
The average weight and height were 62.8 kg (SD±11.5) and 1.56 m (SD±0.09), respectively. The average BMI was 26.0 Kg/m2 (SD±4.6) and stratifying this variable showed that 47 (26.4%) were underweight and 36 (20.2%) were obese.
The MNA indicated that 55.6% of the elderly were at risk of malnutrition and 28.7% were malnourished. Alzheimer's disease was found in 71 (48%) of residents and 14 (7.9%) had PI.
Concerning the diet administered, 113 older adults used oral food and of these, 53 (46.90%) also used food supplements. In terms of mobility, 98 (55.1%) were bedridden, 139 (78.1%) underwent motor physiotherapy and 144 (80.9%) used diapers. The average length of stay at the LCT was 26 months (SD±6-125). Data associated to clinical-nutritional situation and those associated to specific care are described in Table 2.
Table 2: Clinical-nutrition and specific care data from studied elderly (n=178)
BMI: Body Mass Index
kg: kilograms
LS: Length of stay
m: Meters
max: Maximum
min: Minimum
MNA: Mini nutritional assessment score
PI: Presence injury
SD: Standard Deviation
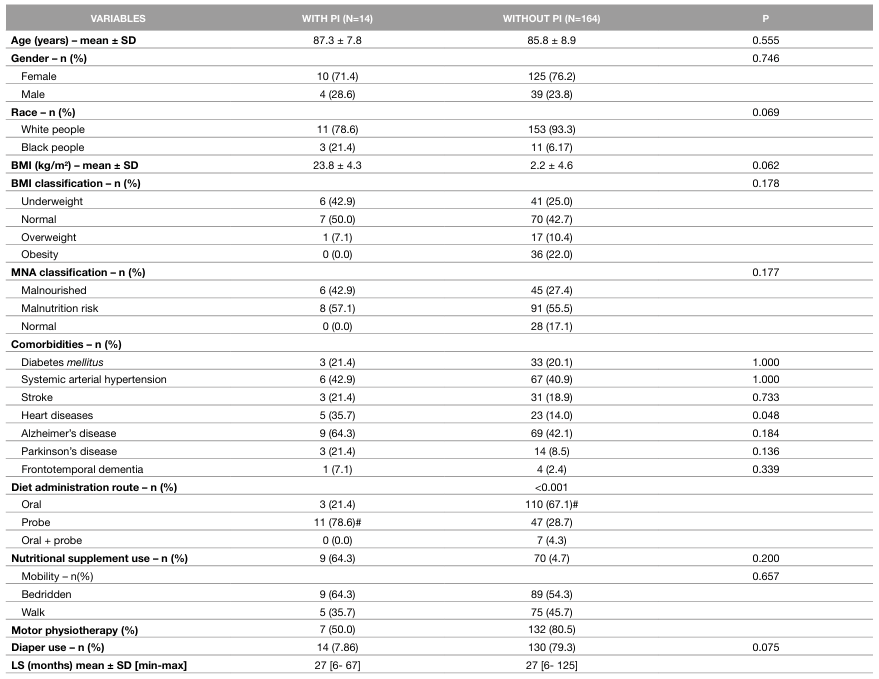
Older adults with PI did less motor physiotherapy (p=0.015), had more heart diseases (p=0.048) and used more tube feeding (p<0.001), as shown in Table 3.
Table 3 : Sociodemographic, clinical, nutritional, specific care and pressure injury association data
# Statistically significant association by the residual test adjusted to 5% significance.
BMI: Body Mass Index
LS: Length of stay
MNA: Mini nutritional assessment score
PI: Presence injury
SD: Standard Deviation
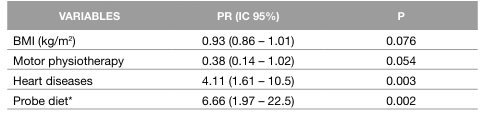
After adjusting for the multivariate model, the presence of heart disease (p=0.003) and the use of a feeding tube (p=0.002) remained significantly associated with the occurrence of PI. Older adults with heart disease had around four times more PI and those who received only tube feeding or tube and oral feeding had 6.66 times more PI when compared to those who received only oral feeding. Table 4 shows the Poisson regression analysis to assess the factors independently associated with PI. Table 4 shows the Poisson regression analysis for assessing factors independently associated to PI.
DISCUSSION OF THE RESULTS
This study presented no association between the PI occurrence and the nutritional status of older adults living in LCT, regardless the method used. This result was also found in a similar study (16). Unlike these results, other studies have shown a significant association between nutritional status, assessed by BMI or MNA, and PI (6, 17-19).
Regarding BMI, 42.9% of the elderly with PI were underweight and 7.1% were overweight. Oliveira, Haack and Fortes (20) found that 29.4% of the elderly with PI were underweight and 19.6% were overweight. Ciríaco et al. (21) found a higher prevalence of overweight (39.5%) in older adults with PI. When we use MAN to identify nutritional status, most of the elderly with PI were at risk of malnutrition ( (55.6%) and 28.7% were already malnourished.
A Brazilian study of 51older adults using the MNA showed that majority of individuals with PI were malnourished (54.5%) and that 27.3% were at risk of malnutrition. This study also found no association between PI and nutritional status (20). Other studies, when using the MNA to define the nutritional diagnosis, found an association between the PI occurrence and nutritional depletion (22-25).
The prevalence of PI in this study was 7.9% and 77.52% of the elderly with PI were aged 80 or over. Similar results were found in a Brazilian study of 69 elderly residents in two LCT, where the authors identified a prevalence of PI of 5.8%, with 50% of residents aged 80 or over (26). In a systematic review published in 2019 on the prevalence of PI in LCT, the authors found a high variation (from 3.4% to 32.4%) (27). We found that the elderly with PI had more heart disease. Rocha et al. (28) indicated the heart disease as one of the most frequent comorbidities in older adults with PI. Studies in LCT in Australia and Canada have shown that hypertension and other heart diseases are risk factors for developing PI (6, 29-31). These diseases alter the blood perfusion of the skin with the possibility of tissue ischemia. The drugs used to treat these conditions can also affect blood flow and make tissues more susceptible to pressure (32).
Among the elderly with PI, 78.6% used a feeding tube. A similar study showed that 75% of the elderly with PI used a feeding tube (26). According to Ciríaco (33) and Campos et al. (34), the need for an alternative route of diet administration indicates that clinical and nutritional frailty should be considered a predictor for the development of PI.
As well, the elderly who were doing motor physiotherapy tended to have less PI. According to Souza and Bertolini (35), the musculoskeletal system is the most affected by immobility, leading to movement limitations that make it impossible to change position, maintain correct postures and transfer beds, which exponentially increases the risk of developing PI.
In this study, it is possible that the nutritional diagnosis was underestimated or overestimated in some situations, since weight and height were estimated using formulas, due to the immobility of the elderly in bed.

