











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
The uterine niche, also called isthmocele, is a recess located in the anterior wall of the uterine isthmus, over the cesarean section scar.1 This condition is often asymptomatic but may be associated with gynecological symptoms such as abnormal uterine bleeding, pelvic pain and secondary infertility.2 Being an entity still little known, its diagnosis is often not made, and these symptoms end up being attributed to an unknown etiology. Its formation is attributed to a post-cesarean gynecological sequel, and taking into account that this surgical procedure has been increasingly frequent in clinical practice,3 it is essential to be alert to this entity.
The diagnostic process begins with the symptomatic evaluation followed by the necessary complementary diagnostic methods. Endovaginal ultrasound is the first-line diagnostic method.4 Other methods may be used, such as hysteroscopy and magnetic resonance imaging.4 Once the diagnosis has been established, it is essential to adapt the treatment to be applied on a case-by-case basis.5 This treatment may include hormonal methods or surgery to remove the uterine recess, and surgical treatment seems to be the most effective in resolving symptoms.1
Case report
A 37-year-old Caucasian woman. No relevant personal history, no usual medication. Non-smoker, she practices regular exercise, daily walks and yoga twice a week.
Their food is based on the Mediterranean diet, with alcohol consumption only socially. Her obstetric history is characterized by a pregnancy and a cesarean delivery at the age of 36 (Fig. 1).
After delivery, the user was observed in the context of a postpartum review consultation at her reference Health Center. At the time of consultation, the user had no loss of lochia and contraception was started with desogestrel 0.075 mg.
Four months later, in a Family Planning consultation at her reference health centre, the user reported complaints of menstrual irregularity and pelvic pain, which she associated with the start of taking oral contraception.
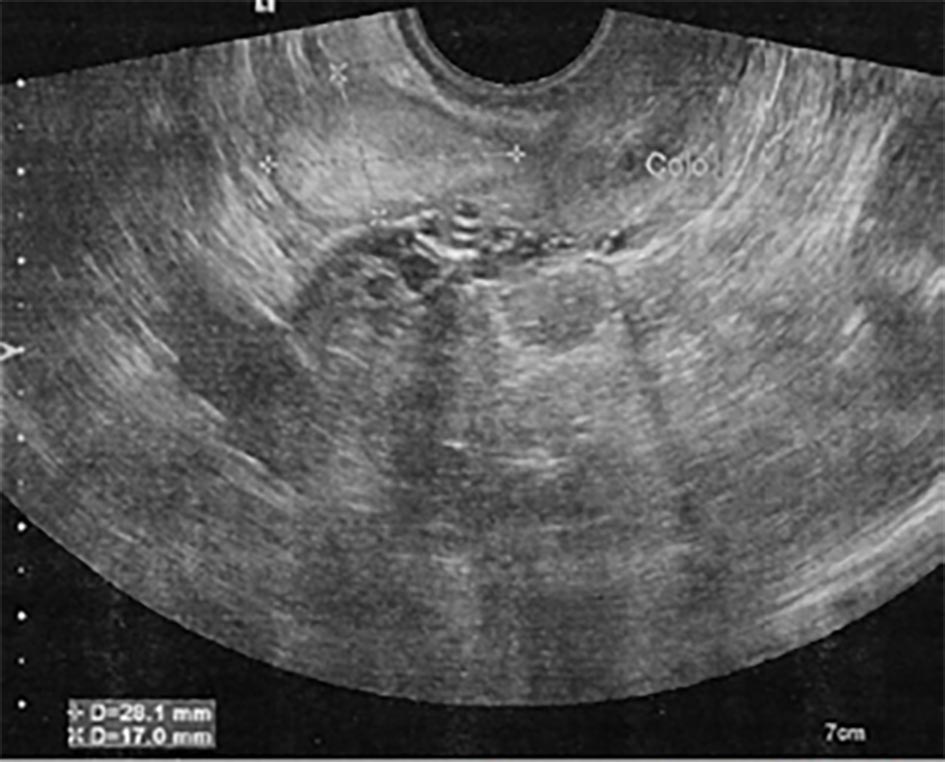
In this consultation, an endovaginal ultrasound was requested to clarify the symptoms and its suspension was advised, using a condom as a contraceptive method until the result of this complementary examination was evaluated. Endovaginal ultrasound revealed “...along the anterior contour of the isthmus, an echogenic oval formation with well-defined limits measuring 28x17 mm axes, with a plane of cleavage with the uterus, in the topography of the cesarean scar.
Ultrasound reassessment was recommended within 4 to 6 months or eventually for better characterization with magnetic resonance imaging”. The image corresponding to this ultrasound is shown in Fig. 2.
Taking into account the recommendation made and the persistence of the complaints, a new ultrasound was performed 6 months later. In a scheduled consultation, the user also reported complaints of pelvic pain, very discreet, like “pricks”, but without significant interference in her daily life. At the time of the consultation, she revealed that she had no intention of becoming pregnant, despite putting this hypothesis in the long term. The result of the new ultrasound was evaluated, which showed “...in the topography of the cesarean scar, the predominantly echogenic oval formation, already identified, dimensionally and morphologically stable.” At this point, in order to improve the symptoms presented by the user, it was necessary to review contraception.
After discussing the possible options and addressing the pros and cons of the various contraceptive methods, the user ended up choosing to start using a vaginal ring.
The present clinical case was discussed with a specialist in Gynecology, who hypothesized the diagnosis of a uterine niche and advised referral to a specialist consultation, a request that was made, with referral to the reference hospital.
In an outpatient Gynecology consultation, which took place about 6 months after the referral by the family physician, the user continued to complain of menstrual irregularities, no longer associated with pain, whose onset was reported in the postpartum period.
The gynecological examination showed no significant alterations and the endovaginal ultrasound performed at the time of consultation was superimposed on those performed previously. After discussing the possible contraceptive methods to be applied in this situation, it ended up being decided to place an intrauterine system with levonorgestrel, which it maintains to date.
About two months after the Gynecology consultation, the user was reassessed in a scheduled consultation at her reference health centre. She was well-adapted to the new contraceptive method, with no complaints of pain or vaginal bleeding. Still without a decision regarding the possible future pregnancy. She referred to a very significant improvement in her quality of life and was really satisfied with the solution found, despite having been two difficult years, due to the symptoms she was reporting. Her sexual activity had improved significantly, with no reported pain complaints.
Discussion
The recognition of the uterine niche is essential, since the rate of cesarean sections has been increasing, and consequently its possible complications. Pelvic pain and menstrual irregularities are common postpartum symptoms being evaluated in primary health care. It is important to understand the cause of these complaints for efficient therapeutic guidance. The uterine niche can be surgically resected via operative hysteroscopy, vaginal surgery, laparotomy/laparoscopy, or a combined approached. Hormonal contraception (oral or IUS) can be an effective alternative to treat the symptoms.

