











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
Stroke is an acute injury, of ischemic or hemorrhagic origin (1), caused by various cerebrovascular diseases, with a high incidence in clinical practice. In Portugal, it was the second leading cause of death during 2019 (2) and, in the following year, it rose to first place, representing 9.2% of the country's mortality (3). National estimates of disability-adjusted years of life lost due to stroke in Portugal, during 2019, were around 1,737.69 per 100 thousand inhabitants (2).
Some stroke survivors spontaneously recover from deficits without intervention or treatment resulting from structural and functional changes in the brain (neuroplasticity)(4). Others present different reversible or permanent neurological manifestations, which can bring cognitive consequences (5,6,7), translated into mild sequelae, insufficient to disturb the person's activities of daily living (ADL's). or lead to a state of unconsciousness, disabling limitations or total dependence.
Post-stroke cognitive impairment (PSCI), present in 20% to 80% of people (8), is defined as a syndrome that encompasses several cognitive deficits, in which memory, attention, executive functions, perception and language are the most affected domains (7,9). This problem predicts a lower quality of life, worsening inability to perform ADL´s and instrumental activities of daily living, higher mortality and institutionalization rates, increased caregiver burden, increased health costs and personal suffering (8,10,11), which becomes a challenge for the healthcare team, including the specialist nurse in rehabilitation nursing (SNRN).
According to the literature, the focus of rehabilitation is on improving post-stroke physical deficits, to the detriment of cognitive deficits (8), although there is evidence that the latter are fundamental to the learning process (5), for planning the rehabilitation environment and return home (10). Adding the fact that cognitive deficits are more difficult to recover than physical ones (12), it is necessary to introduce a cognitive rehabilitation program to people affected by a stroke, for their effective reintegration.
Cognitive rehabilitation is defined as an individualized and structured set of therapeutic activities aimed at restoring cognitive deficits in a domain or global cognitive function, with the aim of minimizing the impact of these deficits on relevant aspects of people/families' lives (13), which is in line with Regulation number 392/2019, when it states that SNRN interventions aim to ensure the maintenance of functional capabilities, improve residual functions and minimize the impact of disabilities installed at the level of neurological function (14).
The cognitive rehabilitation nursing program to the person with stroke must be individualized, with repetitive and systematic interventions, which can address global cognitive function or detected deficits, when the established plan focuses on specific domains of cognition (15), in a way to maximize cognitive capabilities, promote cognitive re-education, in convergence with obtaining health gains (improved psychological well-being, improved functionality in carrying out ADL´s and family and sociocultural reintegration) (14,15,16). The approach must be ensured in interdisciplinarity (2,4,14,17,18), which includes the SNRN, in an involvement coordinated with the person and their goals, family, friends and other caregivers (17), so that they experience a healthy transition, remain or return to their home and community, live in a way adapted to their condition and participate in education, work and civic life (6,19).
To define the timeline for the implementation of interventions that enhance stroke recovery and rehabilitation, we used guidance from the first Stroke Recovery and Rehabilitation Round Table (4). Thus, the aforementioned authors establish four phases: hyperacute phase, which corresponds to the first 24 hours after the event; acute phase, which takes place in the first week post-stroke, in which few studies report restorative interventions; subacute phase: initial (between the seventh day and the third month), period of greater neural plasticity, essential for rehabilitation, which is why interventions aimed at recovery are recommended, and late (between three and six months) and chronic phase, corresponds to the period greater than six months post-stroke.
The approach to people with PSCI remains controversial due to the evidence gap, the scarcity and existence of restrictions and biases in the guidelines written and the scarcity of quality data regarding the ideal approach (13, 20). Based on this assumption, the objective of this study aims to identify cognitive rehabilitation programs for people with stroke.
METHODOLOGY
With the aim of deeply understanding the phenomenon under study (21), synthesizing existing knowledge on a topic and incorporating the results into clinical practice (22), an integrative literature review was carried out. After identifying the theme, the guiding question was defined according to the PICO strategy simplified in PIO (table 1).
Table 1 PIO Strategy
| Participants (P) | Adults with stroke |
|---|---|
| Intervention (I) | Cognitive rehabilitation programs |
| Outcomes (O) | Improved cognitive function |
Source: The Authors
After analyzing the PIO strategy, the following research question was asked: “What cognitive rehabilitation programs are used to improve the cognitive function of people with stroke?”.
In a second phase, the Boolean phrase was constructed, which began with the definition of the Descriptors in Health Sciences/Medical Subject Headings (DeCS/MeSH), used as common language in the search and retrieval of subjects and scientific articles in the Virtual Library sources. in Health and in available databases (23), combined with the Boolean operators AND and OR that define relationships between the search terms and the components of the PICO mnemonic, as represented in table 2.
Table 2 Construction of the Boolean phrase
| Operators Booleans |
AND |
|---|---|
| Concept 1 (P) | ("Stroke" OR "Apoplexy" OR "Cerebral Stroke" OR "Cerebrovascular Accident" OR "Cerebrovascular Apoplexy" OR "Vascular Accident" OR "Cerebrovascular disorders") |
| Concept 2 (I) | ("Nursing Rehabilitation" OR "physiotherap*" OR "therap*" OR "Rehabilitation" OR "Disability Evaluation" OR "Recovery of Function" OR "disabilit*" OR "exercis*" OR "training" OR "Stroke Rehabilitation" OR "Cognition Therapy" OR "Cognitive Behavio*" OR "Therapy" OR "Cognitive Psychotherapy" OR "Cognitive Therapy" OR "Neurological Rehabilitation") |
| Concept 3 (O) | ("Cognitive Dysfunction" OR "Cognitive Decline" OR "Cognitive Impairments" OR "Mental Deterioration" OR "Mild Cognitive Impairment" OR "Mild Neurocognitive Disorder" OR "Cognition Disorders") |
| 1 AND 2 AND 3 | |
Source: The Authors
As a result of this process, the research expression was constructed: (("Stroke" OR "Apoplexy" OR "Cerebral Stroke" OR "Cerebrovascular Accident" OR "Cerebrovascular Apoplexy" OR "Vascular Accident" OR "Cerebrovascular disorders") AND ("Nursing Rehabilitation" OR "physiotherap*" OR "therap*" OR "Rehabilitation" OR "Disability Evaluation" OR "Recovery of Function" OR "disabilit*" OR "exercis*" OR "training" OR "Stroke Rehabilitation" OR "Cognition Therapy" OR "Cognitive Behavio*" OR "Therapy" OR "Cognitive Psychotherapy" OR "Cognitive Therapy" OR "Neurological Rehabilitation") AND ("Cognitive Dysfunction" OR "Cognitive Decline" OR "Cognitive Impairments" OR "Mental Deterioration" OR "Mild Cognitive Impairment" OR "Mild Neurocognitive Disorder" OR "Cognition Disorders")).
An organized and methodical research approach was carried out during the months of November and December 2022, in the scientific databases CINAHL Complete, MEDLINE Complete and MedicLatina, available on the EBSCOhost aggregator, with search limits: publications between 2017-2022 and the languages Portuguese, English and Spanish/Castilian. For the selection of articles, predetermined inclusion/exclusion criteria were applied (Table 3).
Table 3 Inclusion and exclusion criteria for article selection
| Selection criteria | Inclusion criteria | Exclusion criteria |
|---|---|---|
| Participants | - People with stroke - Age over 18 years old |
- Other pathologies |
| Intervention | - Cognitive rehabilitation using technological means - No description of interventions |
|
| Results | - Improved cognitive function | |
| Study design | - Primary studies | - Secondary studies |
Source: The Authors
Articles using technological means were excluded because in some contexts access to technology is still limited. With this review, we sought to focus on practices that are more widely applicable, regardless of technological access.
The initial screening of studies was the responsibility of the main researcher, being subsequently validated by a second researcher, with no need for a third reviewer as no doubts, difficulties or disagreements were found (24). The collection and systematization of data was carried out using various tables.
The selected articles were imported into Microsoft Excel for organization and initial processing. Excel's ‘Remove Duplicates’ function was used to identify and eliminate duplicate entries, ensuring that each study was considered only once in the analysis.
RESULTS PRESENTATION
The research process resulted in 2327 articles of which six articles were included as described in the PRISMA Flowchart (Figure 1).
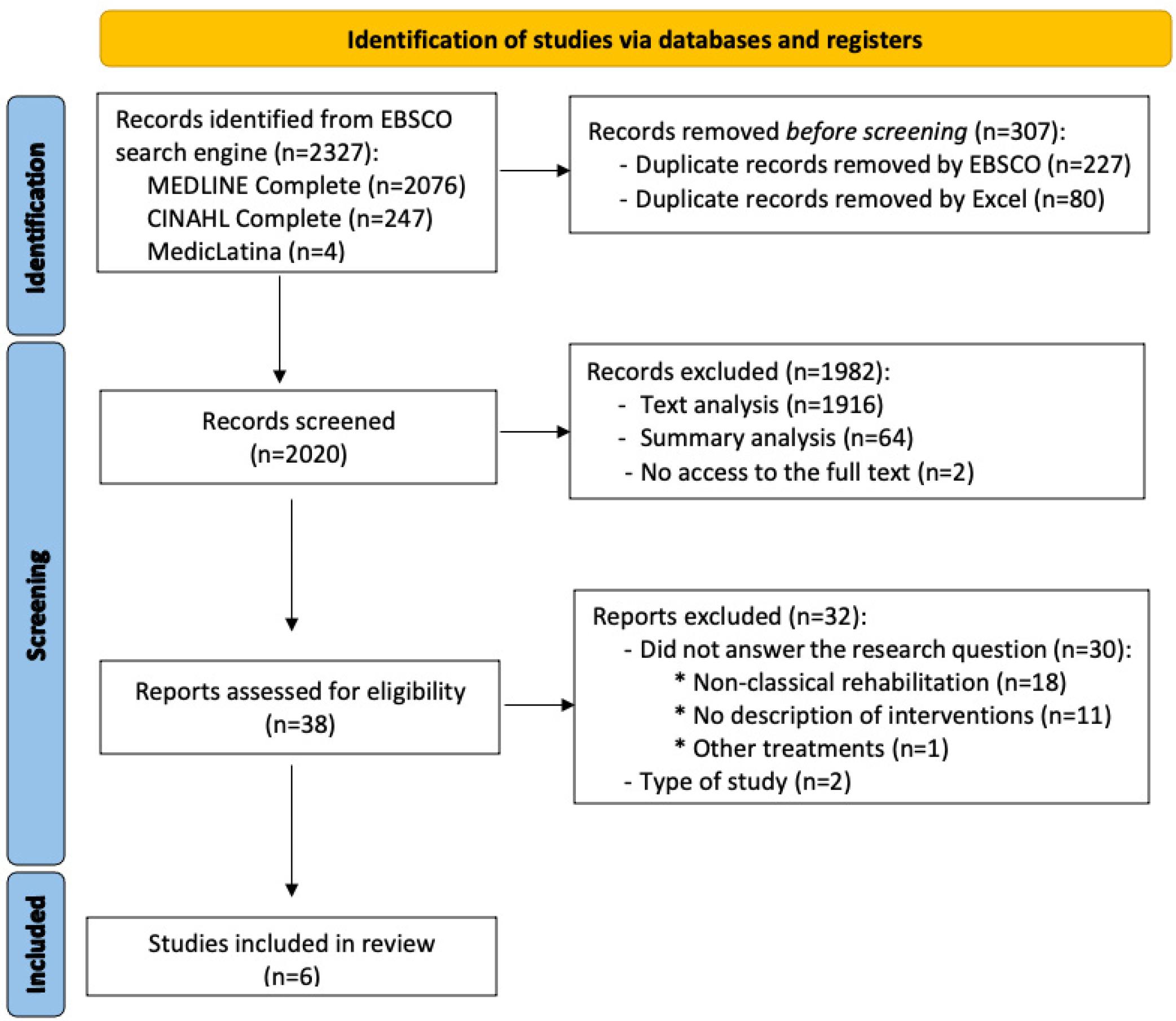
Figure 1 PRISMA flowchart - Research and study selection process. Source: The Authors, adapted (25).
Articles without access to the full text were excluded only after access attempts had been exhausted and searched on other platforms, databases and/or requested from the authors via email.
The articles mainly comprise randomized clinical trials (RCT) (n=4), a clinical trial with a control group (n=1) and a quasi-experimental study with a control group (CG) (n=1). All selected articles are published in scientific journals and written in English. The years of publication on the topic under study date back to 2021 (n=4) and 2022 (n=2). China is the country that concentrates the majority of studies (n=5), followed by Iran (n=1), as for Portugal, there is no study that meets the objectives of this integrative literature review (ILR).
The population subject to interventions is mostly male, which corroborates a higher incidence of the disease in this population and the average age varies between 53.9 and 66.8 years, showing a higher incidence in direct relation to the increasing age (26,27). Three of the studies portray only ischemic stroke as this type of stroke represents 80-85% of all strokes (28), with the predominance of strokes of ischemic etiology being evident in two studies (16,29) in relation to the predominance of hemorrhagic etiology, found only in one study (11).
The programs found are carried out either individually (n=3) or in group sessions (n=3), the latter reported in one of the cognitive rehabilitation articles and in the two RT studies.
Of the studies included, four identify the SNRN as intervening health professionals, one study (11) does not discriminate the professional category, referring to professionals as rehabilitation therapists and the other study (28) does not specify the professional group that intervenes in cognitive rehabilitation for people with stroke.
In order to organize, synthesize and interpret the results obtained from the review (22), it was decided to present the data in tables according to year, authors and study design (table 4), summarize the data extracted from the studies (table 5) and present the cognitive rehabilitation programs found (attached in Supplemental material).
Table 4 Identification of included studies.
| Study | Authors. Title (Year) | Study design |
|---|---|---|
| A | Jiang, H., Li, H.,Wang, Z., Xiaomei, X., Su, Q. & Ma, J. Effect of Early Cognitive Training Combined with Aerobic Exercise on Quality of Life and Cognitive Function Recovery of Patients with Poststroke Cognitive Impairment (2022). |
RCT |
| B | Li, A. & Liu, Y. Reminiscence therapy serves as an optional nursing care strategy in attenuating cognitive impairment, anxiety, and depression in acute ischemic stroke patients (2022). |
RCT |
| C | Xuefang, L., Guihua, W. & Fengru, M. The effect of early cognitive training and rehabilitation for patients with cognitive dysfunction in stroke (2021). |
RCT |
| D | Pashang, S., Zare, H., Alipour, A. & Sharif-Alhoseini, M. The effectiveness of cognitive rehabilitation in improving visual and auditory attention in ischemic stroke patients (2021). |
Quasi-experimental (pre-intervention, post-intervention and follow-up design) and CG. |
| E | Wang, H., Zhu, C., Liu, D., Wang, Y., Zhang, J., Wang, S. & Song, Y. Rehabilitation training improves cognitive disorder after cerebrovascular accident by improving BDNF Bcl-2 and Bax expressions in regulating the JMK pathway (2021). |
RCT |
| F | Cheng, C., Fan, W., Liu, C., Liu, Y., & Liu, X. Reminiscence therapy-based care program relieves post-stroke cognitive impairment, anxiety, and depression in acute ischemic stroke patients: a randomized, controlled study (2021). |
RCT |
Table 5 Summary of data extracted from studies included in the ILR.
| Study | Objective | Participants | Intervention | Results | Conclusions |
|---|---|---|---|---|---|
| A | Explore the effect of early cognitive training combined with aerobic exercise on the recovery of cognitive function in people with PSCI. | 90 participants: experimental group (EG) (n=45) and CG (n=45). | People in the CG received conventional health education combined with rehabilitation training and those in the EG received early cognitive training combined with aerobic exercise. | The GE scored higher on the Montreal Cognitive Assessment (MoCA) test. | Early cognitive training combined with aerobic exercise promotes recovery of cognitive function. |
| B | To explore the effect of RT on cognitive impairment in people with stroke. | 216 people, randomized into reminiscence therapy group (RTG) and CG (1:1 ratio) | The CG underwent conventional motor and cognitive rehabilitation interventions and the RTG underwent the same interventions with additional RT. | The RTG had a higher Mini Mental State Examination (MMSE) score at 9 and 12 months and a lower cognitive impairment rate per MMSE at 12 months, compared to the CG. | RT impairs cognitive impairment, indicating its potential to manage post-stroke. |
| C | Explore the effects of early cognitive training and rehabilitation for people with cognitive dysfunction in stroke. | 118 people, divided into observation group (n=59) and CG (n=59). | Both groups received conventional cognitive rehabilitation training. | After 4 weeks, the CG achieved a significant improvement in the MoCA score and a reduction in the values on the National Institutes of Health Stroke Scale (NIHSS). | Active nursing intervention in the early cognitive rehabilitation of people with post-stroke cognitive impairment is of great importance, in order to restore function, reduce complications and improve quality of life. |
| D | Investigate the effectiveness of a cognitive rehabilitation program in improving visual and auditory attention performance in people with stroke. | 20 people randomly classified into EG (n=10) and CG (n=10). | The CG underwent a routine rehabilitation program and the EG underwent the same program, plus a cognitive rehabilitation program. | The cognitive rehabilitation program improved the domains of auditory attention by 67% and visual attention by 23% in people in the EG. | The cognitive rehabilitation program improved related cognitive functions with attention to people with stroke. |
| E | Explore the effect of rehabilitation training on post-stroke cognitive impairment. | 100 participants were divided into CG (n =50) and research group (n =50). | CG participants received routine medication and people in the research group received rehabilitation training based on routine drug therapy. | 6 months later, MoCA and MMSE test scores were significantly higher in the research group than in the CG. | Rehabilitation training can improve the mental state and cognitive level of people with stroke. |
| F | Evaluate the benefit of a RT-based care program in restoring CC in people with acute ischemic stroke. | 130 participants were randomized into RTG or CG, in a 1:1 ratio. | CG participants received cognitive rehabilitation training and RTG underwent the same interventions, with additional RT. | The MMSE score and MoCA score of the RTG increased and the percentage of people with CC assessed by the MoCA test reduced at 12 months, compared to the CG. | A RT-based program may help reduce CC in people with acute ischemic stroke. |
Considering ethical aspects, at ILR we aim to ensure the referencing of researched articles and follow the rules at all stages, in order to avoid bias and minimize errors (31). As it is a ILR that does not directly involve human beings, approval of the research project by the Research Ethics Committee was not necessary.
DISCUSSION
REHABILITATION PROGRAMS IN THE ACUTE PHASE
The post-stroke acute phase covers the largest number of articles found in this ILR (n=3). All included studies relating to this phase are RCTs and reveal positive results on cognitive function in people with cognitive impairment, regardless of the type of interventions reported, the way they were implemented or the beginning, duration and number of sessions that determined the program implemented. The authors of study A (11) enhanced the recovery of cognitive function through an aerobic exercise program combined with early cognitive training implemented in people with cognitive impairment after a first-time stroke. This is a study whose EG is made up of 90 people who obtained a higher MoCA score compared to the CG made up of the same number of participants.
Study B (30) reflects the comparative results of an observation group of 59 people and a CG with the same number of people diagnosed with ischemic stroke for the first time. Both groups underwent a conventional rehabilitation program but, while the observation group was subjected to a movement observation therapy program using virtual reality equipment, the latter were subjected to an additional conventional cognitive rehabilitation program. In this case, the interest of the investigation in this ILR is on the CG, which achieved improvements in the MoCA score and reduction in values on the NIHSS scale, although lower than the observation group.
In study C (16), the effect of rehabilitation training on post-stroke cognitive impairment is explored and improvements were obtained in the MoCA and MMSE test in the research group made up of 50 people in relation to the CG, made up of the same number of participants.
The authors of study A (11) refer to rehabilitation therapists as professionals responsible for implementing the rehabilitation programs under study, without distinction of professional category, while the remaining two studies mentioned highlight the SNRN intervention.
All the studies mentioned above addressed interventions aimed at rehabilitating deficits in attention, orientation, perception and memory, although the first two also addressed language.
There is great heterogeneity in relation to the frequency and duration of rehabilitation programs carried out: the study A (11) included sessions once a day, six times a week and lasting six months, the clinical trial C (16) lasted 60 minutes, twice a day lasting three weeks while the study E(29) carried out the program once a day for half an hour and each treatment cycle lasted eight weeks.
In all studies there was concern about stabilizing vital signs, with the authors of study C (16) starting the program on the third day post-stroke, without there being progression of stroke symptoms for two days and those of study E (29) between 72 hours and the sixth day post-stroke.
The studies included in this review mostly used the MoCA test to reassess cognitive deficits; however, the study E (29) concomitantly used the MMSE test. Regarding the timing for the reassessment of deficits, while the study A (11) and the study E (29) refer to the six months, the study C (16) mention the 14th and 20th day post-intervention. Since cognitive rehabilitation is comprehensive and aimed at various cognitive domains, it was decided to group the different approaches aimed at them, in order to facilitate their understanding and discussion.
Attention
All studies address the rehabilitation of attention deficits in people affected by stroke and report the beginning of early rehabilitation, even during hospitalization.
As for the interventions carried out, these differ between studies. In studies A (11) and E (29), the interventions involve showing photographs according to the person's preference and guiding them to describe the objects found in them, but they differ in other points: while the first ones add interventions of repeating positive and negative numbers, as well as of the even and odd numbers, from one to thirty, the second read stories/poetry and ask the person to retell them. The study E (29) use simple games as an intervention for attention rehabilitation.
Memory
Three articles were found that present rehabilitation programs for memory deficits, with some disparity in the proposed interventions. The studies A (11) and C (16) propose remembering names or guiding people to retell a story, helping people remember the characters or objects they have just seen.
Study A (11) researchers help recall recent events to enable the person to solve problems and perform simple tasks independently (dressing, undressing, and washing their face) with the help of family members, while those in study E (29) help people identify colors, shapes, and names with cards, building blocks, pictures, alarm clocks, schedules and diaries, remember the time and rehabilitate calculation (inserted in working memory) through card games.
Executive Functions
In the studies included, executive functions include the ability to solve problems, the ability to reason and thought disorders. Thus, to improve the ability to solve problems, study C (16) propose organizing the materials necessary to carry out ADL´s, to enable the person to complete them independently. To improve people's reasoning ability, study E (29) proposes classifying and solving practical problems, such as encouraging people to decide on the type and quantity of daily meals, going to stores near the hospital to select and buy items/negotiate with sellers. Regarding study A (11), in order to recover from thought disorders, people were encouraged to leave and return to the ward or order food independently.
Perception
For the rehabilitation of perception, proposed in studies A (11) and E (29), people were encouraged to recognize/distinguish the shape or color of objects. In the second study mentioned, they add that people remember the names of characters represented in photographs.
Language
In order to rehabilitate language-related deficits, the study A (11) and C (16) converge in dialogue on subjects of interest to the person, raising questions. The second also included repeated listening with reading and retelling of stories as rehabilitation interventions in this domain.
Orientation
Program in this area is seen at an early stage in three of the studies. Briefly, in the study A (11) and C (16) have in common the questioning about the time, place and date and differ in the interventions: while in the first study they frequently remember the time to get up and go to bed and train calculation operations within the range numerical from zero to fifty, the second allows the distinction between the laterality of the limbs, position and distance between hospital objects. The study E (29) requires the person to remember the route between the ward and the treatment room and the time of ADL´s.
REHABILITATION PROGRAMS IN THE SUBACUTE PHASE
Although both studies refer to the presence of acute stroke, they do not specify the time elapsed from the event to the start of the program, which begins after hospital discharge. In this way, the subacute phase is considered.
Reminiscence Therapy
It is a non-pharmacological procedure that promotes remembering the past and sharing experiences and stories, in order to promote cognitive functions (30). This approach was found in two articles in the present review. Both studies were carried out on people with acute ischemic stroke and comprised 60-minute sessions starting after hospital discharge, taught by nurses who had undergone specific prior training. The duration of both programs was 12 months, but the frequency differed: while in study B (30) the sessions were held once a month, in the study F (12) sessions took place twice a month. In the study B (30), the 108 participants in the RTG underwent a program that included motor rehabilitation and cognitive rehabilitation, in addition to RT and in the study F (12), RTG participants were 65 and performed a cognitive rehabilitation program with additional RT.
In summary, the RT programs consisted of remembering/recalling events and sharing past experiences, feelings and thoughts with the nurses and the rest of the group participants. Although there were some differences in the intervention, both groups achieved improvements in their scores on the MMSE test in relation to the CG and the second was also evaluated with the MoCA test, also showing improvement in this item.
To explain the improvement in cognitive function observed in study B (30), the researchers point to the exercise of memory through remembering the past, experiences and stories and the organization of language to share memories and feelings, while in study F(12) they conclude that RT associated with cognitive rehabilitation strengthens memory, orientation, association and narrative capacity, which is why both suggest RT as a complement to the global rehabilitation of people with acute ischemic stroke. In both studies, cognitive function was assessed every three months throughout the program. Although, in study B (30), only the MMSE test was applied, in study F (12), the MoCA test was simultaneously applied to carry out the reassessment of deficits and justify the results of the studies.
REHABILITATION PROGRAMS IN THE CHRONIC PHASE
The D study (28) refers to the chronic phase of the stroke (period between six months and three years after the stroke), the period considered in the definition of chronic stroke. The particularity of this article is related to cognitive rehabilitation with prospects for improving the domain of attention, both visual and auditory.
This is a quasi-experimental study with the participation of 20 people with ischemic stroke, randomly allocated to CG (n=10) and EG (n=10). The interventions were carried out in groups of two to ten people, lasting one hour per week over eight weeks and the content of the sessions included clarifications on attention deficits and several training sessions in this area. The reassessment of the attention domain was carried out through the Continuous Integrated Visual and Auditory Performance Test at the end of the program and six weeks after its end.
CONCLUSIONS
This ILR made it possible to identify cognitive rehabilitation programs in the various phases of stroke recovery (acute, subacute and chronic phase), which allows us to conclude that cognitive rehabilitation, despite promoting more evident clinical improvements in the first two phases, in which predicts greater neural plasticity, which can also be seen months or years after the injury (32).
Cognitive rehabilitation points to an improvement in results in the domains of cognition or global cognitive function, translated into an improvement in the scores of the tests applied, demonstrating the importance of the role of the SNRN in the interdisciplinary approach to people with stroke.
It is crucial to screen PSCI, even if they are not immediately apparent. The MoCA test is the instrument most used in studies to assess cognitive deficits, which demonstrates its applicability and sensitivity in people with cognitive impairment during a stroke.
In any case, some limitations were found:
● Weakly structured programs, with no consensus regarding the beginning, frequency and duration of the programs found, the evaluation time and the type of interventions applied;
● There is no evidence that participants' personal characteristics influence or not the effectiveness of interventions;
● No studies were found aimed at the European population, particularly the Portuguese population;
● Heterogeneity of interventions for different cognitive domains;
● The timings for evaluating results are divergent;
● Some of the studies compared the effectiveness of cognitive rehabilitation interventions with interventions not targeting cognitive function;
● Both the participants' initial assessment and the results are mainly related to the MoCA and MMSE test overall, but do not specify the results obtained in the different cognitive domains.
Despite PSCI being of great concern to the person/family and its identification as a high priority area for future research, there are several gaps and a lack of high-quality data that allows for an ideal proposal of intervention, confirmed by others authors (13). Therefore, the need for more studies in this area is highlighted, including methodologically robust trials, in order to meet these needs.
Despite the limitations highlighted, the study brought a body of knowledge in the area of cognitive rehabilitation that allows it to support the intervention of SNRN, in order to promote evidence-based practice on the part of these professionals, improving the quality of care provided to the person with PSCI. These professionals are essential in bridging the gap between clinical assessment and practical, ongoing rehabilitation efforts, ensuring patients receive comprehensive care tailored to their evolving needs. They assess cognitive function and develop a personalized cognitive rehabilitation program tailored to the specific deficits identified, with the goal of facilitating recovery.

