











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
The majority of submandibular space infections have an odontogenic etiology1. Gram-positive anaerobic cocci are the most frequently isolated microorganisms2. The aerobic and gram-positive bacillus Listeria monocytogenes (Lm) is responsible for a food-borne illness named listeriosis3. In healthy individuals, it typically presents as a relatively non-severe self-limiting gastrointestinal infection. However, among patients with underlying risk factors such as extremes of age, pregnancy and immunosuppression it can be more severe, presenting as meningitis and bacteremia3. Focal invasive infections with abscess formation are rare, manly as a consequence of hematogenous seeding or direct inoculation4. Typically, they are only diagnosed after the culture results become available5. We aim to present a case report of a rare focal manifestation of this infection, in accordance with the CARE reporting checklist6.
Case report
A 75-year-old male, with a history of chronic alcohol abuse, abstinent for the past month, and no regular medication, presented to our institution with a 3-week history of progressing pain and submandibular swelling. On physical examination, the patient also presented with paralysis of the mandibular branch of the facial nerve and a decayed single tooth on the lower left quadrant. His body temperature was 37.5ºC, and all the other vital signs were within normal range. A contrast-enhanced computed tomography (CT) revealed a 1,7cm submandibular abscess, with parapharyngeal extension (Figure 1). From blood analysis it was possible to do the inaugural diagnosis of type 2 diabetes mellitus (T2DM). A transcervical incision and drainage of the abscess was performed, and empirical intravenous treatment with amoxicillin plus clavulanic acid 1,2g 8/8 hours (h) and clindamycin 600mg 8/8h was started.
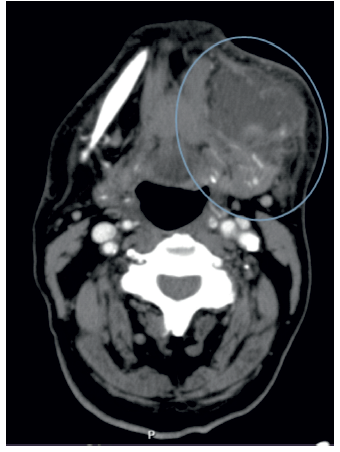
Figure 1 Emergency department CT scan: Axial section contrast-enhanced CT scan performed in the emergency department, demonstrating a 1,7cm submandibular abscess.
During hospitalization, an extraction of the root remnant in the third quadrant was performed. Blood cultures were negative. From the drained pus culture, Lm was isolated, and a mandatory notification has been made. At this time, a new anamnesis was carried out, with further deepening of social history, but there was no consumption of suspicious food. According to the antibiotic sensitivity test results, a targeted antibiotic therapy with intramuscular G-penicillin 24MU/day was initiated 13 days after admission. At this point, there was a clinical and imagiological significant improvement revealed by a new CT scan (Figure 2).
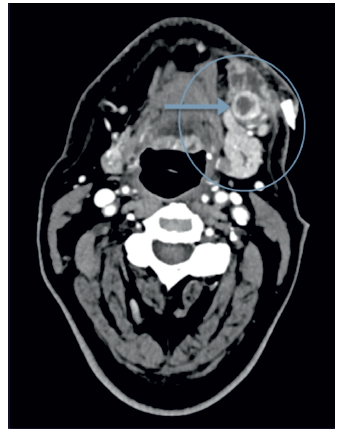
Figure 2 Hospital stay CT scan: Axial section contrast-enhanced CT scan performed on the 13th day of hospitalization, demonstrating improvement of submandibular abscess and an abscessed ganglion (arrow).
After 16 days, the patient was discharged home on oral amoxicillin 1g 8/8h, over a 10-day period, with good adherence and tolerability. In follow-up appointments, a complete resolution of the infection was observed, however, the patient remained with sequalae of mandibular branch paralysis. Furthermore, the patient started treatment with metformin 850mg/day plus a basal-bolus insulin therapy and was referred to the general practitioner (GP) for further follow-up.
Discussion
Although the annual rate of sporadic listeriosis in Europe and North America is less than 1 per 100,000 population per year, this infection remains underdiagnosed3. As listeriosis has an unusual clinical presentation and morphological resemblance with other bacteria, the true prevalence remains unknown7),(8. The bacteria Lm is ubiquitous, leading to common contamination of the surface of meat and vegetables, at a rate of up to 15%3. It is most frequently found in dairy products and processed meat7. In this case, the source of infection was not found.
As mentioned before, focal invasive infection is rare. There are clinical cases describing endocarditis, myocarditis, pericarditis, arteritis, pneumonia, pleuritis, cholecystitis, peritonitis, liver/spleen abscess, brain abscess, breast abscess, arthritis, osteomyelitis, sinusitis, otitis, lymphadenitis, necrotizing fasciitis, conjunctivitis, and endophthalmitis7),(9. However, as far as our literature search could determine, only 3 articles mention unequivocally the presence of a cervical abscess4.
A recent systematic review described 19 culture-proven cases of Lm lymphadenitis, of which 44% had evidence of suppuration4. Taking into account the image results of our patient, we cannot exclude lymph node involvement. Given the negativity of blood cultures, the most probable route of infection is seeding from a locoregional portal of entry4. Therefore, in this clinical case, the submandibular abscess most probably results from an extension of the periodontal infection. The predominant cervical involvement may be explained by a translocation in the mucosa-associated lymphoid tissue of the pharyngo-oral region4.
The immune response to Lm is cell-mediated, which means that conditions leading to T-cell suppression predispose to listeriosis. They include malignancies, HIV infection, chronic alcohol abuse, T2DM, extremes of age, and pregnancy9. Our patient had three risk factors, age over 65 years, chronic alcohol abuse and T2DM. According to Blot et al. (4, the reported prevalence of this last disease among patients with lymphadenitis by Lm is 67%, being T2DM the most common associated risk factor. The same authors4 also highlighted the importance of evaluating for the presence of neoplasia, since it had a prevalence of 22%.
The first-line therapy against Lm is penicillin or ampicillin, alone or combined with an aminoglycoside. Alternatively, it can be administered trimethoprim-sulfamethoxazole10. In persons allergic to penicillin, vancomycin combined with an aminoglycoside may be used10. The administration of cephalosporins, quinolones, chloramphenicol, erythromycin and tetracycline should be avoided9. By consensus, treatment should last for 3 weeks or more10. In this case, the patient was initially treated empirically for 13 days, and then the antibiotics were switched to a targeted therapy for more 13 days.
Infections within the submandibular space can spread into the neck and mediastinum, making the involvement of this region very dangerous2. Also, the mortality rate associated with listeriosis ranges from 20% to 30%10. These high values can be explained by a combination of immunocompromised patients and a delayed diagnosis3.
In conclusion, given its impact in public health, rarity, and high mortality rate, listeriosis is a notifiable disease. This clinical case highlights the need to drain abscesses, culture pus samples, and test antimicrobial susceptible patterns to treat the disease correctly and effectively. Although very rare, we must think of Lm in the presence of a cervical abscess. Moreover, it is extremely important to control the identified risk factors.
Conflicts of interest
The authors declare that there is no conflict of interests regarding the publication of this paper.
Data confidentiality
The authors declare having followed the protocols in use at their working center regarding patients’ data publication.
Privacy Policy, Informed Consent, and Ethics Committee Authorization
The authors declare that they have obtained written consent for the use of patient information in this article.

