











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Crohn’s disease (CD) is a chronic transmural inflammatory bowel disease that usually affects the distal ileum and colon, but may occur in any part of the gastrointestinal tract. Extraintestinal manifestations (EIM) occur in up to 40% of patients and can significantly impact the quality of life of patients with CD, sometimes more so than the intestinal disease1,2. They most commonly affect the musculoskeletal system, skin, hepatobiliary tract and eyes, but as a systemic disease almost any organ can be involved. In up to 25% of patients a first EIM develops before the onset of CD and, while some of them may occur or aggravate in relation to intestinal flares, others may present an entirely independent course from underlying disease activity1,2. Colonic involvement and perianal disease seem to confer a higher risk of associated EIMs1,2.
Oral manifestations have been reported to range widely from 5% to 50%, but seem to be more prevalent in the pediatric population2-4. These can be divided in specific and non-specific manifestations with the difference lying in the granulomatous substrate of specific manifestations5,6. Non-specific manifestations include aphthous ulcers/aphthous stomatitis, perioral erythema, angular cheilitis or periodontitis. These are reported to be more common and tend to follow the course of the underlying CD1,2,4. Specific manifestations are rarer and include cobblestoning of the mucosa, deep linear ulcerations, hyperplastic mucogingivitis and mucosal tags4,6. Another specific feature that can appear years before a proper diagnosis of CD is granulomatous cheilitis present in orofacial granulomatosis (OFG).
OFG is a complex condition that results from granulomatous infiltration of the orofacial tissues, particularly the lips, with no evidence of systemic involvement. It is found in less than 1% of patients with CD, taking the name of orofacial CD (OCD), a form of metastatic CD4,6. Its mainstay is the recurrent to persistent lip swelling, but other specific lesions are usually associated and sometimes facial palsy or cervical lymphadenopathy may also be present2-4,6. It often follows a chronic and disfiguring course and does not usually parallel intestinal disease activity, making it exceptionally difficult to manage4.
Nasal and paranasal manifestations are even rarer. The first description of these was made in 1985 by Kinnear7. Since then, very few other cases have been reported in the worldwide literature, each with different clinical presentations and treatments7-17. Sinonasal complaints may be of nasal obstruction, crusting, bleeding, purulent rhinorrhea or acute or chronic sinusitis. Septal perforation, saddle nose, atrophic rhinitis, necrosis of the turbinates and stenosis of the nasal fossae have all been reported as possible findings.
Ear involvement encompasses both the external and inner ear. External ear manifestations are usually considered extensions of other concurrent conditions of broader skin involvement, like pyoderma gangrenosum (PG) or cutaneous metastatic CD2,18. Inner ear was considered for a long time as an immune-privileged site thanks to the role of the blood-labyrinthine barrier, but over the years a growing interest for immune-mediated inner disease has developed19. Autoimmune inner ear disease (AIED) is considered primary when the inner ear is the only affect organ, but in up to 30% patients with AIED it is secondary to a systemic autoimmune disease20. Autoimmune reactivity to the inner ear has been reported as a clinical feature in a number of systemic immune-mediated disorders, including inflammatory bowel disease, but mostly in cases of ulcerative colitis (UC) (18,19,21. The clinical expression of AIED can be heterogenous, particularly in cases of secondary AIED, but in most cases it shows a bilateral and asymmetrical sensorineural hearing loss that is rapidly progressive over a period of several weeks or months. Frequently, in the early stages, only one ear can be affected and hearing thresholds can fluctuate, with periods of deterioration alternating with periods of remission20. In about 50% of AIED patients, hearing loss is also associated with vestibular symptoms, such as imbalance and motion intolerance, ataxia and positional or episodic vertigo18,20,22. Diagnosis of this condition is essentially based on clinical presentation, high responsiveness to immunosuppressive drugs such as corticosteroids and exclusion of other possible causes.
Case reports
Case 1
Female patient, 31 years old, diagnosed with ileocolic CD for six years. Since the beginning with recurrent aphthous stomatitis associated with intestinal flare-ups. Approximately one year after initiating follow-up, started exhibiting significant clinical worsening with frequent cortico-dependent exacerbations requiring hospitalization. In this context, biologic therapy was started, but she showed a primary non-response to Adalimumab and was switched to Infliximab, achieving clinical and endoscopic remission after an initial need for dose and interval optimization. A few months later, she started complaining of nasal obstruction, crusting and vestibular fissuring with recurrent vestibulitis, along with persistent angular cheilitis (Fig. 1). These symptoms responded to corticosteroid and antibiotic therapy (topical or oral as needed), but recurred upon treatment suspension. Relapse of her oral aphthae (Fig. 2) and worsening intestinal symptoms followed and a loss of response to Infliximab was assumed. As a result, she was switched again to Ustekinumab. Since then, she has achieved near-complete remission of all manifestations (intestinal, oral and nasal). Currently, she only experiences mild perioral and perinasal dryness and scaling, which she manages with local hygiene and hydration measures as needed.

Case 2
Female patient, 58 years old, diagnosed with colonic CD for five years and with secondary enteropathic spondyloarthropathy for four years. Clinical, endoscopic and biochemical remission was initially achieved under a triple regimen with Sulfasalazine, Methotrexate and Infliximab. After about two years, she appeared with worsening of her extraintestinal manifestations (EIMs) - including articular exacerbation, episodic episcleritis and new onset of persistent nasal pruritus, crusting and anterior nasal septal perforation (Fig. 3). In this context, a loss of response to Infliximab was assumed and she was switched to Adalimumab with complete clinical remission across all EIMs. Approximately six months later, she developed recurrent episodes of intense nasal pruritus followed by sudden edema of the upper lip with variable extension to the left hemiface and eyelid. Over time, the episodes become more frequent and durable with gradual installment of a persistent and firm lip edema (Fig. 4). The case was discussed in a multidisciplinary setting, considering angioedema associated with Adalimumab versus metastatic CD as differential diagnoses. A trial of Adalimumab discontinuation was undertaken, but no regression of symptoms occurred after drug washout. A labial biopsy was performed, confirming the diagnosis of OCD. From a therapeutic perspective, each isolated episode initially responded to systemic corticosteroid therapy, but only during the treatment period. There was no response to maintenance therapy with topical corticosteroids or calcineurin inhibitors. Consequently, intralesional corticosteroid administration was attempted, achieving partial clinical remission. The patient is currently awaiting authorization for a new biologic switch.

Case 3
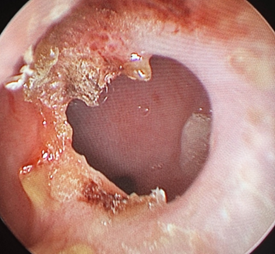
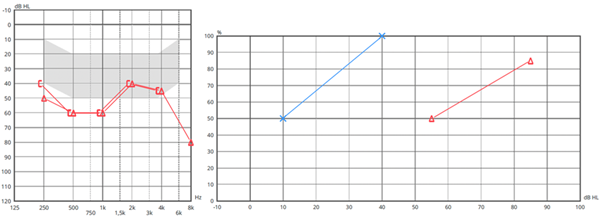
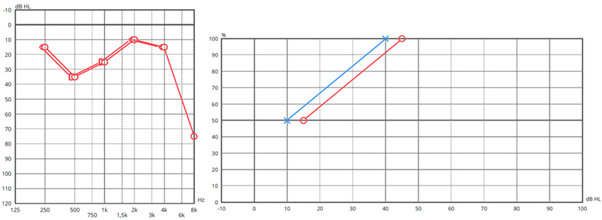
Female patient, 29 years old, diagnosed with CD for four years. Around 6 months after initial diagnosis, she developed rapidly progressive gait imbalance and bilateral aural fullness and hearing loss, without vertigo. An oral corticosteroid regimen was started with stabilization of the symptoms, but no significant improvement and she was later admitted to the hospital for further investigation and treatment. Among the complementary diagnostic tests performed, the following findings stood out: (1) audiogram with bilateral sensorineural hearing loss at the frequency extremes, (2) Video Head Impulse Test (vHIT) with reduced gains in all six canals bilaterally, (3) videonystagmography (VNG) with bilateral areflexia and (4) positive anti-68kD antibody. Cranioencephalic and ear magnetic resonance imaging (MRI), lumbar puncture and additional autoimmune and serologic workup showed no abnormalities. During hospitalization, she underwent multiple sessions of plasmapheresis and pulses of methylprednisolone with improvement in auditory symptoms. She was discharged on oral corticosteroid therapy and referred for vestibular rehabilitation (VR) and follow-up in Neurology and Otorhinolaryngology outpatient clinics. Post-hospitalization, there was no significant recovery of gains on vHIT, but there was progressive improvement in balance symptoms with VR. From a hearing perspective, symptoms recurred when attempting to taper oral corticosteroids, leading to the initiation of Azathioprine. Since then, she started experiencing episodic right-sided auditory fluctuations, which were managed with on-demand intratympanic corticosteroid therapy (Fig. 5). Approximately 6 months ago, due to a progressive increase in episode frequency, along with worsening gastrointestinal symptoms, a multidisciplinary decision was made to increase the dose of Azathioprine. Since then, no further episodes have occurred and hearing has stabilized (Fig. 6).
Discussion
This case series highlights the diversity of ENT manifestations of CD and underscores the complexity of diagnosing and managing these conditions. Each case presents a different pattern of otorhinolaryngological involvement - ranging from granulomatous cheilitis in the context of OFG, different forms of nasal disease and AIED - illustrating the known yet underrecognized associations between CD and ENT manifestations.
While oral aphthous ulcers are relatively common in CD, the rarity of granulomatous cheilitis/OCD poses significant diagnostic challenges, as seen in Case 21-6. Similarly, nasal involvement, as observed in Cases 1 and 2, is also exceedingly rare and associated with highly variable and non-specific findings that can easily mimic other ENT-specific conditions or systemic diseases, such as Wegener’s granulomatosis 7-17.
These cases reinforce the importance of considering CD in patients presenting with chronic oral/perioral and nasal inflammatory conditions, especially in highly steroid-responsive cases. The fact that some of these lesions and conditions can even precede a formal CD diagnosis or be a first manifestation of loss of response to therapy makes it that more crucial for clinicians to have a high suspicion index for the possibility of these associations.
Furthermore, while some of these manifestations tend to parallel intestinal activity and are usually managed in conjunction with the underlying disease (Case 1), others may require specific treatments or the need to consider underlying treatment escalation, even in the absence of intestinal exacerbations (Case 2).
Case 3 brings attention to the underexplored association between AIED and CD. Although AIED is more commonly associated with UC than with CD18,19,21, inner ear involvement in systemic autoimmune diseases is increasingly recognized19. The pathophysiology of AIED involves immune-mediated damage to cochleovestibular structures and manifests as rapidly progressive bilateral, but often asymmetrical sensorineural hearing loss associated with variable vestibular dysfunction. Early stages, like in Case 3, can often present with unilateral fluctuating symptoms that may mimic primary inner ear disorders, such as Menière’s disease20. However, presence of concomitant systemic autoimmune conditions and episodes of simultaneous bilateral affection, like in Case 3’s presenting episode, may help in the differentiating between the two.
Our patient also presented with positive anti-68kD antibodies and showed a highly steroid-responsive disease course. Although the absence of these antibodies doesn’t necessarily dismiss a diagnosis of AIED, previous reports have linked their presence to an autoimmune etiology of inner ear disease, as well as correlated them to the disease’s degree of steroid-responsiveness18,22,23. Literature also suggests that tumor necrosis factor (TNF) plays a critical role in AIED pathogenesis with higher levels found in patients with AIED when compared to healthy subjects, particularly in the subset of patients that were steroid-resistant. In this context, and although the patient in question is currently stable after an increase in Azathioprine dosage, if biologic therapy should need to be initiated down the line, anti-TNF drugs might provide added benefit18,22,24.
Conclusion
Overall, all these cases reinforce the need for a comprehensive understanding of both the specific characteristics of each manifestation and their interaction with the underlying CD, making multidisciplinary cooperation key for the proper management of these patients. Given the growing recognition of immune-mediated otorhinolaryngological complications in IBD, particularly CD, further research might be warranted to clarify their pathogenesis, optimize therapeutic strategies and improve patient outcomes.
Conflito de interesses
Os autores declaram que não têm qualquer conflito de interesse relativo a este artigo.
Confidencialidade dos dados
Os autores declaram que seguiram os protocolos do seu trabalho na publicação dos dados de pacientes.
Proteção de pessoas e animais
Os autores declaram que os procedimentos seguidos estão de acordo com os regulamentos estabelecidos pelos diretores da Comissão para Investigação Clínica e Ética e de acordo com a Declaração de Helsínquia da Associação Médica Mundial.

