










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.21 no.5 Lisboa out. 2014
https://doi.org/10.1016/j.jpg.2014.06.002
ENDOSCOPIC SPOT
An uncommon presentation of a rare disease in the gastrointestinal tract
Uma apresentação invulgar de uma doença rara no tracto gastrointestinal
Joana Moleiroa,∗, Paulo Bernardob, Sandra Faiasa, António Dias Pereiraa
a Serviço de Gastrenterologia do Instituto Português de Oncologia de Lisboa Francisco Gentil, EPE, Portugal
b Serviço de Hematologia do Instituto Português de Oncologia de Lisboa Francisco Gentil, EPE, Portugal
*Corresponding author
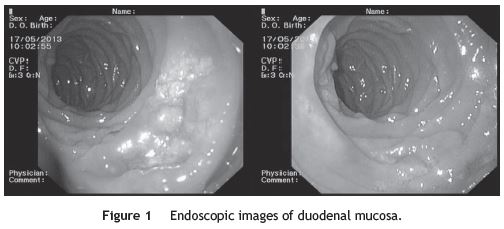
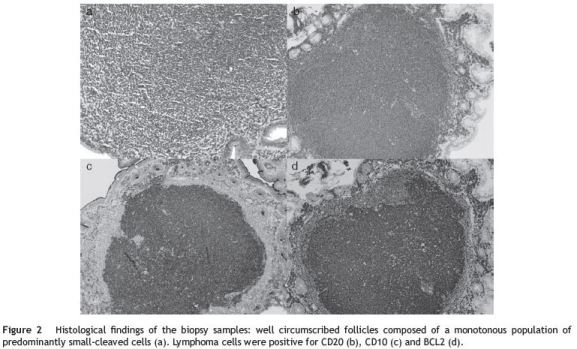
A 57-year-old caucasian man with no remarkable medical history was evaluated for an iron deficiency anemia recently detected in routine blood tests. He denied blood loss, epigastric discomfort, nausea, vomiting, changes in bowel habits, weight loss or fever. Physical examination revealed no abnormalities, namely hepatosplenomegaly or peripheral lymphadenopathy. An esophagogastroduodenoscopy (EGD) was performed with evidence of an ulcerated lesion with irregular, elevated and slightly whitish fundus and borders measuring 25mm at the second portion of duodenum (Fig. 1). Other three smaller lesions with similar endoscopic appearance were visualized in the second and third portion of the duodenum. Biopsy specimens showed well-circumscribed follicles composed of a monotonous population of predominantly smallcleaved cells that were positive for CD20, CD10 and BCL-2 (Fig. 2), but negative for CD5. A grade 1-2 follicular lymphoma was diagnosed, according to the World Health Organization classification.1 An ileocolonoscopy was also performed, which revealed no abnormalities. The computed tomography scan of the thorax, abdomen and pelvis was normal and the bone marrow biopsy had no abnormalities. According to the Ann Arbor System Classification2 the lymphoma was in stage IEA. Based on iron deficiency anemia, the patient was submitted to chemotherapy, a total of eight cycles of R-CVP (rituximab, cyclophosphamide, vincristine and prednisolone) without complications, except for fingers paresthesias that determined vincristine dose reduction in the last three chemotherapy cycles. After treatment, EGD was repeated, without any duodenal alterations. Resolution of anemia was also achieved.
The gastrointestinal (GI) tract is the most common site of extra-nodal non-Hodgkins lymphoma (NHL), accounting for 30-40% of all primary extranodal NHL. The stomach is the most common primary site, followed by the colorectal region and the terminal ileum. The most frequent histologic subtypes of GI-NHL are mucosal-associated lymphoid tissue (MALT) lymphoma or high-grade B cell lymphoma.3 Primary GI follicular lymphoma (PGI-FL) is a rare disease accounting only about 1-3.6% of all GI non-Hodgkin lymphomas. Although the duodenum and terminal ileum are still considered its most common location, the development of wireless capsule endoscopy and double balloon enteroscopy has increased the detection of PGI-FL in all segments of the small intestine. Approximately 80% of patients are estimated to have multiple lesions throughout the entire GI tract.4
The representative endoscopic feature is well known to be small whitish polypoid nodules lesions up to 2mm in diameter.4 Herein we present a case of primary duodenal follicular lymphoma with multiple predominantly ulcerated lesions as the main endoscopic feature, with the largest lesion presenting elevated, whitish and irregular borders and fundus.
The median age of patients at diagnosis of PGI-FL is 56 years old, with a female predominance. Most patients are asymptomatic (43%), with lesions incidentally detected during routine EGD. When symptoms are present, they include abdominal pain, GI obstruction or bleeding.4
There is still no consensus regarding the treatment modality for PGI-FL. The first line treatment may be radiotherapy, surgical resection, systemic chemotherapy, monoclonal antibody monotherapy, a combination of these therapies, or a watch and wait policy depending on patients symptoms.5
References
1. Jaffe ES. The 2008 WHO classification of lymphomas: implications for clinical practice and translational research. Hematol Am Soc Hematol Educ Prog. 2009;1:523-31. [ Links ]
2. Rohatiner A. Report on a work shop convened to discuss the pathological and staging classifications of gastrointestinal tract lymphoma. Ann Oncol. 1994;5:397-400. [ Links ]
3. Nakamura S. B cell lymphoma of the small intestine. In: Bosman FT, Carneiro F, Hruban RH, Theise DT, editors. WHO classification of tumours of the digestive system. 4th ed. Lyon-France: International Agency for Research on Cancer; 2010. p. 69-73. [ Links ]
4. Yamamoto S. Gastrointestinal follicular lymphoma: review of the literature. J Gastroenterol. 2010;45:370-88. [ Links ]
5. Kodama M. Primary follicular lymphoma of the gastrointestinal tract: a retrospective case series. Endoscopy. 2008;40:343-6. [ Links ]
*Corresponding author
E-mail address: joana moleiro@hotmail.com (J. Moleiro).
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent. The authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Received 22 April 2014; accepted 11 June 2014


{kind=link}