










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.22 no.4 Lisboa ago. 2015
https://doi.org/10.1016/j.jpge.2015.03.004
ENDOSCOPIC SNAPSHOT
Aspiration of Capsule Endoscopy
Aspiração de Cápsula Endoscópica
Pedro Magalhães-Costa∗, Miguel Bispo, Cristina Chagas
Gastroenterology Department, Hospital Egas Moniz, Centro Hospitalar de Lisboa Ocidental, Lisbon, Portugal
* Corresponding author.
Keywords: Capsule Endoscopy/adverse effects
Palavras-chave: Endoscopia por Cápsula/efeitos adversos
1. Case description
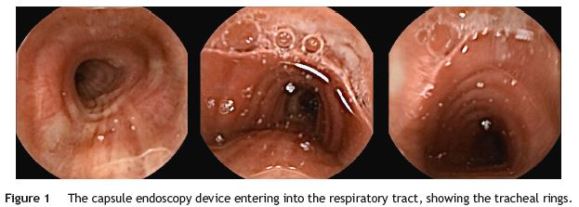
A 92-year-old man was referred to our endoscopy department for overt obscure gastrointestinal bleeding (OGIB) investigation, thus a capsule endoscopy (CE) - PillCam@ SB2 (Given Imaging Ltd., Yoqneam, Israel) was performed. As comorbidities, he had Parkinson disease and diabetes mellitus. The patient had no prior history of dysphagia or cerebrovascular events and the device was ingested under the surveillance of an experienced nurse. No complaints were mentioned at the time CE was ingested. Four hours later, the patient felt a sudden dyspnea compelling him to a vigorous cough. After some minutes the CE device was expelled intact and the patient, asymptomatic, returned the device to our department. The recorded video photograms showed that the device was persistently in the mouth and pharynx of the patient for almost four hours and then entered the trachea (Fig. 1). The typical features of this structure are easily recognizable (the incomplete cartilaginous rings anteriorly and laterally, and a straight membranous wall posteriorly).
CE is considered a safe and effective method for studying OGIB.1 Although, as with any other medical diagnostic device, it is not devoid of potential complications. Our case presents a very rare but potentially fatal complication. After the first reported case in 2003, only 25 cases are described in the literature2 and most of them had a spontaneous resolution, after vigorous cough. Older patients and those with neurological diseases are prone to such complication and, as recommended by some authors, very old patients and those with known dysphagia or neurological diseases should have the device introduced via a delivery system (simple net or the AdvanCE delivery device).3 Recently, the Real-Time Viewer4 was introduced with the aim of inform, in real-time, the clinician where is the device and if a delivery system or a prokinetic should be employed to aid the passage to the small-bowel. Physicians and their teams should identify these patients at higher risk of CE aspiration in order to prevent a potentially fatal outcome.
References
1. Fisher L, Lee Krinsky M, Anderson MA, Appalaneni V, Banerjee S, Ben-Menachen T, et al. The role of endoscopy in the management of obscure GI bleeding. Gastrointest Endosc. 2010;72:471-9. [ Links ]
2. Koulaouzidis A, Rondonotti E, Karargyris A. Small-bowel capsule endoscopy: a ten-point contemporary review. World J Gastroenterol. 2013;19:3726-46. [ Links ]
3. Tóth E, Fork FT, Almqvist P, Thorlacius H. Endoscopy-assisted capsule endoscopy in patients with swallowing disorders. Endoscopy. 2004;36:746-7. [ Links ]
4. Gao YJ, Ge ZZ, Chen HY, Li XB, Dai J, Ye CA, et al. Endoscopic capsule placement improves the completion rate of small-bowel capsule endoscopy and increases diagnostic yield. Gastrointest Endosc. 2010;72:103-8. [ Links ]
* Corresponding author.
E-mail address: pmagalhaescosta@gmail.com (P. Magalhães-Costa).
Ethical disclosures
Protection of human and animal subjects. The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent. The authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interest
The authors have no conflicts of interest to declare.
Authors contribution
Pedro Magalhães-Costa is the author guarantor. The manuscript is approved by all Authors. All authors have contributed to and agreed on the content of this manuscript. Pedro Magalhães-Costa wrote the manuscript, Pedro Magalhães-Costa and Miguel Bispo diagnosed, treated and followed the patient, Cristina Chagas critically revised the manuscript.
Received 17 March 2015; accepted 18 March 2015

