










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.22 no.5 Lisboa out. 2015
https://doi.org/10.1016/j.jpge.2015.03.010
ENDOSCOPIC SNAPSHOT
Anal Pain and Constipation - Beyond the Obvious
Proctalgia e Obstipação - Para Além do Óbvio
Sandra Barbeiro∗, Catarina Atalaia Martins, Pedro Marcos, Cláudia Gonçalves, Bruno Arroja, Manuela Canhoto, Liliana Eliseu, Filipe Silva, Isabel Cotrim, Helena Vasconcelos
Gastroenterology Department, Centro Hospitalar de Leiria, Leiria, Portugal
* Corresponding author.
Keywords: Anal Canal; Constipation; Foreign Bodies; Pain
Palavras-Chave: Canal Anal; Corpos Estranhos; Dor; Obstipação
1. Case report
An 85-year-old male developed constipation after orthopaedic surgery and was treated with oral laxatives and enemas. After starting the medication he complained of anal pain and rectal bleeding. The primary care physician diagnosed an anal fissure and prescribed anal ointments.
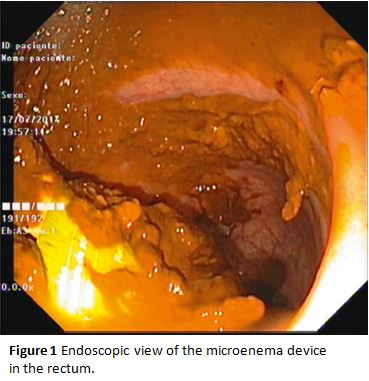
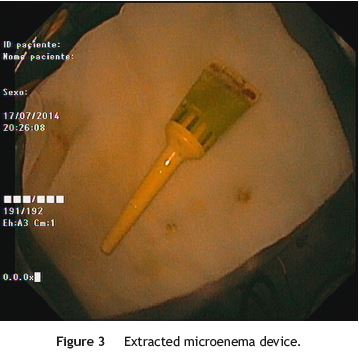
As pain became more severe he came to our hospital for observation. When asked, the patient admitted a single use of rectal microenema one month before and digital rectal examination revealed a foreign body within the rectal ampulla. Endoscopic examination of the rectum identified a microenema device (Figs. 1 and 2), which was removed with an anoscopy and a foreign body forceps with addition of a Valsalva manouver by the patient (Fig. 3). No sedation was needed because of the distal localization of the object and good tolerability to the procedure. No complications were registered and the patient was rapidly symptoms free.

2. Discussion
Most rectal foreign bodies are introduced consciously by persons seeking sexual stimulation.1,2 In our case the patient incorrectly applied the microenema and did not give that information to the physicians as he believed he had used it properly. We point out the fact that the foreign body remained in the rectum for a month before it was brought to attention to health care providers. Most objects can be removed transanally.3 In clinically stable patients without evidence of perforation or peritonitis, the rectal foreign body can be removed in the emergency department.3,4 The management depends on the texture, size, shape and location of the object.4 If the foreign body can be easily palpated, it is possible to be extracted transanally using one of many clamps and instruments, with or without direct visualization through a rigid or flexible endoscope.3-5 Open surgery should be reserved only for patients with perforation, peritonitis or impaction of the foreign body.4,5
References
1. Yildiz SY, Kendirci M, Akbulut S, Ciftci A, Turgut HT, Hengirmen S. Colorectal emergencies associated with penetrating or retained foreign bodies. World J Emerg Surg. 2013;8:25. [ Links ]
2. Desai B. Visual diagnosis: Rectal foreign body: a primer for emergency physicians. Int J Emerg Med. 2011;4:73. [ Links ]
3. Goldberg JE, Steele SR. Rectal foreign bodies. Surg Clin N Am. 2010;90:173-84. [ Links ]
4. Coskun A, Erkan N, Yakan S, Yıldirim M, Cengiz F. Management of rectal foreign bodies. World J Emerg Surg. 2013;8:11. [ Links ]
5. Cologne KG, Ault GT. Rectal foreign bodies: what is the current standard. Clin Colon Rectal Surg. 2012;25:214-8. [ Links ]
* Corresponding author.
E-mail address: sandrabarbeiro@gmail.com (S. Barbeiro).
Conflicts of interest
The authors have no conflicts of interest to declare.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Received 28 February 2015; accepted 30 March 2015

