










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.24 no.2 Lisboa abr. 2017
https://doi.org/10.1159/000450876
IMAGES IN GASTROENTEROLOGY AND HEPATOLOGY
Blue Rubber Bleb Nevus Syndrome: A Delayed Diagnosis
Síndrome de Blue Rubber Bleb Nevus: Um Diagnóstico Tardio
Artur Sérgio Gião Antunes, Bruno Peixe, Horácio Guerreiro
Gastroenterology Department, Centro Hospitalar do Algarve, EPE, Faro, Portugal
* Corresponding author.
Keywords: Gastrointestinal neoplasms; Blue nevus, diagnosis; Skin neoplasms
Palavras-Chave: Neoplasias gastrointestinais; Neoplasias da pele; Nevo azul
An 80-year-old woman was referred to our department following a positive fecal occult blood test .From her medical record, we noted a long-standing rheumatoid arthritis. She was chronically treated with methotrexate, prednisolone, and pantoprazole. No relevant family history was recorded.
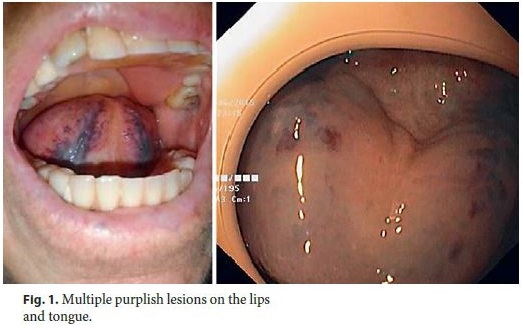
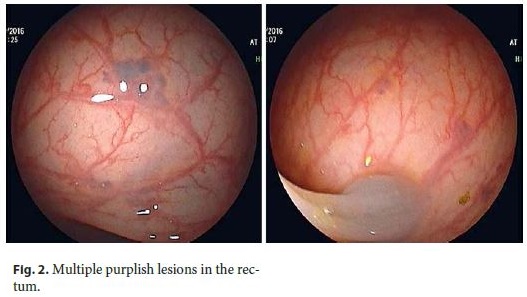
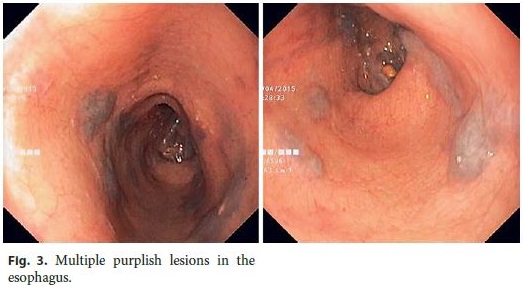
Physical examination revealed multiple nonpulsatile nodular purplish lesions on her lips and tongue surface, easily compressible and promptly refilled afterwards (Fig. 1). The lesions were present since childhood and although they grew in size, they only troubled the patient in rare episodes of self-limiting bleeding secondary to trauma. Laboratory tests were normal. She underwent a colonoscopy and an upper endoscopy and we noticed multiple purplish lesions of similar characteristics in the rectum (Fig. 2), hypopharynx, and esophagus (Fig. 3), without stigmata of recent hemorrhage, but not in the colon, stomach, or duodenum. The characteristics of these lesions were consistent with hemangiomas. Smallbowel video capsule endoscopy also revealed multiple hemangiomas in the jejunum and distal ileum.
We assumed the diagnosis of a multifocal venous vascular malformation, with cutaneous and gastrointestinal involvement. A computed tomography of the brain, chest, abdomen, and pelvis was performed, showing no other vascular malformations or bone deformities with the exception of those in the cervical spine consistent with rheumatoid arthritis.
Given the clinical and imagiological features, we established the diagnosis of a sporadic type of blue rubber bleb nevus syndrome (BRBNS). BRBNS is a rare syndrome and should be considered in the presence of multifocal hemangiomas, preferably in the skin and gastrointestinal tract. BRBNS should be differentiated from other syndromes that occur with cutaneous and visceral vascular malformations, like Rendu-Osler-Weber, Klippel-Trenaunay, and Maffucci syndromes. Its pathogenesis is poorly understood. A family association has already been identified (linked to chromosome 9p), although sporadic type is the commonest. In most cases, hemangiomas are asymptomatic and symptoms are usually the result of its mass effect or rupture with bleeding [1–4].
There is no standard of care for BRBNS. Its treatment should be determined by the topography of lesions and the severity of the disease. In cases of minor or intermittent bleeding, conservative treatment with iron supplementation and blood transfusions are usually enough. In cases of significant bleeding or other complications such as rupture, intestinal torsion, and intussusception, surgical resection or endoscopic sclerosis and laser photocoagulation endoscopic treatment should be considered. Antiangiogenic agents such as corticosteroids, propranolol, interferon-α, octreotide, and sirolimus were successfully used as rescue treatment, although there are some doubts concerning sustained long-term effects [1–4].
References
1 Jin XL, Wang ZH, Xiao XB, Huang LS, Zhao XY: Blue rubber bleb nevus syndrome: a case report and literature review. World J Gastroenterol 2014;20:17254–17259. [ Links ]
2 Choi KK, Kim JY, Kim MJ, Park H, Choi DW, Choi SH, et al: Radical resection of intestinal blue rubber bleb nevus syndrome. J Korean Surg Soc 2012;83:316–320. [ Links ]
3 Rodrigues D, Bourroul ML, Ferrer AP, Monteiro NH, Gonçalves ME, Cardoso SR: Blue rubber bleb nevus syndrome. Rev Hosp Clin Fac Med Sao Paulo 2000;55:29–34. [ Links ]
4 Domini M, Aquino A, Fakhro A, Tursini S, Marino N, Di Matteo S, et al: Blue rubber bleb nevus syndrome and gastrointestinal haemorrhage: which treatment? Eur J Pediatr Surg 2002;12:129–133. [ Links ]
Statement of Ethics
Protection of human and animal subjects: The authors declare that no experiments were performed on humans or animals for this study. Confidentiality of data: The authors declare that no patient data appear in this article. Right to privacy and informed consent: The authors declare that no patient data appear in this article.
Disclosure Statement
The authors have no conflicts of interest to declare.
* Corresponding author.
Dr. Artur Sergio Giao Antunes
Gastroenterology Department, Centro Hospitalar do Algarve, EPE
Rua Leao Penedo
PT–8000-386 Faro (Portugal)
E-Mail sergiogiao@hotmail.com
Received: June 26, 2016; Accepted after revision: August 8, 2016

