










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.25 no.1 Lisboa fev. 2018
https://doi.org/10.1159/000479973
ORIGINAL ARTICLE
Performance of the Choledocholithiasis Diagnostic Score in Patients with Acute Cholecystitis
Performance do score diagnóstico de coledocolitíase em doentes com colecistite aguda
Catarina Gouveia, Rui Loureiro, Rosa Ferreira, Alexandre Oliveira Ferreira, António Alberto Santos, Maria Pia Costa Santos, Carolina Palmela, Marília Cravo
Serviço de Gastrenterologia, Hospital Beatriz Ângelo, Lisbon, Portugal
* Corresponding author.
ABSTRACT
Introduction: The prevalence of choledocholithiasis among patients with acute cholecystitis is estimated to be between 9 and 16.5%. There are no validated algorithms to predict choledocholithiasis in this group of patients. Aim: The aim of this study was to evaluate the performance of the choledocholithiasis diagnostic score proposed by the American Society for Gastrointestinal Endoscopy, in patients with acute cholecystitis. Material/Methods: A retrospective cross-sectional study, covering a 4-year period at a secondary care hospital, was performed. All patients with an encoded diagnosis of acute cholecystitis and with at least one of the following procedures were included: endoscopic retrograde cholangiopancreatography (ERCP), endoscopic ultrasound, magnetic resonance cholangiopancreatography, and intraoperative cholangiography. Results: Among 4,369 patients with the diagnosis of acute cholecystitis, 40 (0.92%) had clinical or sonographic suspicion of choledocholithiasis. Their mean age was 68.1 ± 15 years, and 22 (55%) were men. Thirty-one of the patients included (77.5%) had a high risk of choledocholithiasis, and 9 (22.5%) had an intermediate risk. In 16 (51.6%) of the 31 patients with a high risk, the diagnosis of choledocholithiasis was confirmed. In 2 (22.2%) of the 9 patients with an intermediate risk, the diagnosis of choledocholithiasiswas also confirmed. The high risk score for choledocholithiasis had a positive predictive value of 52% and a sensitivity of 89%. The intermediate risk score for choledocholithiasis had a positive predictive value of 22% and a sensitivity of 11%. Discussion and Conclusions: Suspicion of choledocholithiasis in patients with acute cholecystitis was a rare event (<1%). The sensitivity of the high risk score was approximately the same as found in published series with patients with suspected choledocholithiasis overall (86%), while the positive predictive value was substantially lower (52 vs. 79.8%). Therefore, in patients with acute cholecystitis and suspected choledocholithiasis, this score should not be used to screen for common bile duct stones, and a sensitive method should be used prior to ERCP.
Keywords: Choledocholithiasis, Acute cholecystitis, Endoscopic retrograde cholangiopancreatography
RESUMO
Introdução: A prevalência de coledocolitíase em doentes com colecistite aguda é estimada entre 9 e 16.5%. Não existem algoritmos validados para o diagnóstico de coledocolitíase neste grupo de doentes. Objectivo: Avaliar a performance do score de coledocolitíase proposto pela American Society for Gastrointestinal Endoscopy , em doentes com coleciste aguda. Material/Métodos: Foi realizado um estudo retrospectivo transversal, durante um período de 4 anos num hospital de cuidados secundários. Foram incluídos todos os doentes com diagnóstico codificado de colecistite aguda e pelo menos um dos seguintes procedimentos: colangiopancreatografia retrógrada, ecoendoscopia, colangiopancreatografia por ressonância magnética e colangiografia intra-operatória. Resultados: Em 4,369 doentes com diagnóstico de colecistite aguda, 40 (0.92%) tiveram suspeita clínica ou ecográfica de coledocolitíase. A idade média foi 68.1 ± 15 anos e 22 (55%) eram homens. Dos doentes incluídos, 31 (77.5%) tinham score elevado de coledocolitíase e 9 (22.5%) tinham score intermédio. Em 16/31 (51.6%) doentes com score elevado o diagnóstico de coledocolitíase foi confirmado. Em 2/9 (22.2%) doentes com score intermédio foi também confirmada coledocolitíase. O score elevado de probabilidade de coledocolitíase teve um valor preditivo positivo de 2% e uma sensibilidade de 89%. O score intermédio de probabilidade teve um valor preditivo positivo de 22% e uma sensibilidade de 11%. Discussão e Conclusões: A suspeita de coledocolitíase em doentes com colecistite aguda foi um evento raro (<1%). A sensibilidade do score elevado de probabilidade foi semelhante ao reportado na literatura (86%), mas o valor preditivo positivo foi significativamente menor (52 vs. 79.8%). Assim, em doentes com colecistite aguda e suspeita de coledocolitíase este score não deve ser utilizado, devendo ser realizado um método de diagnóstico antes da CPRE.
Palavras-Chave: Coledocolitíase, Colecistite aguda,·Colangiopancreatografia retrograde endoscópica
Introduction
The prevalence of choledocholithiasis among patients with acute cholecystitis remains controversial. While some studies have reported an incidence of common bile ducts stones (CBDS) from 9.1 to 16.5% of patients presenting with acute cholecystitis [1, 2], others did not find any relation between acute cholecystitis and choledocholithiasis [3]. A diagnosis of CBDS in these patients is a clinical challenge, since liver tests are already altered by the inflammatory process of the gallbladder [4] and the sensitivity of abdominal ultrasound (US) for choledocholithiasis detection is suboptimal [5, 6].
An elevated bilirubin level at the time of diagnosis of acute cholecystitis raises the issue of whether the patient should have an endoscopic retrograde cholangiopancreatography (ERCP) before surgery. Erroneously, clinicians frequently use the choledocholithiasis score, which has been neither developed nor validated for this population. In fact, in 2010 the American Society for Gastrointestinal Endoscopy (ASGE) published a probability score to assess patients with suspected choledocholithiasis [7], which has shown a reasonable diagnostic accuracy (59–62%) [8].
The purpose of this study was to evaluate the diagnostic performance of the ASGE choledocholithiasis score in patients with acute cholecystitis. The score assigns patients a low (<10%), intermediate (10–50%), or high (>50%) likelihood of choledocholithiasis based on clinical predictors. These are stratified into very strong (CBDS on transabdominal US, clinical ascending cholangitis, and a bilirubin level >4 mg/dL), strong (a dilated common bile duct on US and a bilirubin level of 1.8–4 mg/dL), and moderate (abnormal liver biochemical test result other than for bilirubin, age >55 years, and clinical gallstone pancreatitis). According to an algorithm also presented in those guidelines [7], patients with high probability scores should undergo ERCP, while patients with intermediate probability scores should undergo preoperative endoscopic US (EUS), magnetic resonance cholangiopancreatography (MRCP), intraoperative cholangiography (IOC), or laparoscopic US.
Materials and Methods
We conducted a retrospective, single-center, cross-sectional study covering a 4-year period from February 2012 to January 2016 at a secondary care hospital (Hospital Beatriz Ângelo, Lisbon, Portugal). We included all patients with an encoded diagnosis of acute cholecystitis and with at least one of the following complementary diagnostic and/or therapeutic procedures: ERCP, EUS, MRCP, and IOC. The ERCPs were performed by 3 gastroenterologists (A.A.S., R.L., and R.F.). The patients were then stratified into groups at intermediate or at high risk for choledocholithiasis according to the ASGE score. We considered a positive ERCP or positive IOC the gold standard for choledocolithiasis. For each parameter of the score a χ 2 test was performed to evaluate the association with the presence of choledocholithiasis. The sensitivity, specificity, and positive predictive values of the scores for this population were calculated. The statistical analysis was performed using SPSS v23.0.
Definitions
The diagnosis of acute cholecystitis was considered for patients presenting with right upper abdominal pain or tenderness, fever, elevated inflammatory parameters, and evidence of gallbladder stones and a thickened, edematous gallbladder on abdominal US or CT. The diagnosis of cholangitis was established by the presence of Charcots triad (right upper abdominal pain, fever, and jaundice). Biliary pancreatitis was considered for patients with abdominal pain, a 3-fold or higher raise in serum lipase or amylase activity, and the presence of gallstones on CT or abdominal US in the absence of any history or laboratory or radiological findings indicating another etiology of pancreatitis.
Results
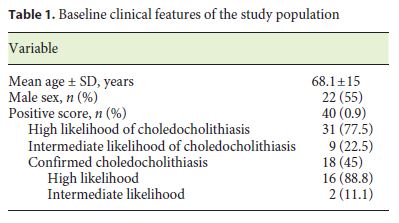
Among 4,369 patients with a diagnosis of acute cholecystitis, 40 (0.92%) had clinical or sonographic suspicion of choledocholithiasis. Their mean age was 68.1 ± 15years, and 22 (55%) were men. All patients with suspected choledocholithiasis had high or intermediate probability scores.
The final sample included the 40 patients with a high or intermediate probability of choledocholithiasis. The baseline clinical features of our study population are shown in Table 1. Thirty-one of the patients included (77.5%) had a high likelihood of choledocholithiasis (HLC) and 9 (22.5%) had an intermediate likelihood of choledocholithiasis (ILC).
Twenty-five (80.6%) of the 31 patients with HLC were submitted to successful ERCP, which confirmed the presence of a CBDS in 15 patients (60%). Of the 10 patients with no evidence of CBDS on ERCP, only 1 had choledocholithiasis confirmed by IOC, which was performed 15 days after the ERCP. In the remaining 6 HLC patients, cannulation of the common bile duct was not achieved, mainly due to an altered anatomy. All of these patients had progressive lowering of bilirubin levels and normalization of liver tests, and thus further ERCP attempts were not made. Overall, the diagnosis of choledocholithiasis was confirmed in 16 (51.6%) of the patients with HLC.
Of the 9 patients with ILC, 7 underwent MRCP, which showed CBDS in only 1 patient, confirmed later by ERCP; the other 6 patients had no evidence of choledocholithiasis on MRCP and had progressive lowering of bilirubin levels and liver function tests. Two patients underwent ERCP, which confirmed CBDS in only 1 of them. Overall, the diagnosis of choledocholithiasis was confirmed in 2 (22.2%) of the patients with ILC.
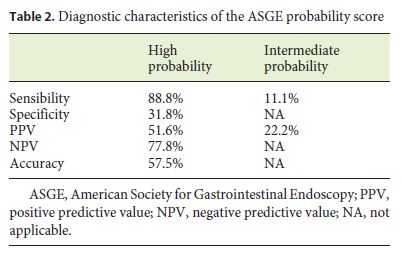
Of the patients included, 25 (63%) underwent total cholecystectomy during the following 30 days. The stratification of HLC had a positive predictive value of 52% and a sensitivity of 89%, while that of ILC had a positive predictive value of 22% and a sensitivity of 11%. Table 2 shows the diagnostic characteristics of the ASGE probability score.
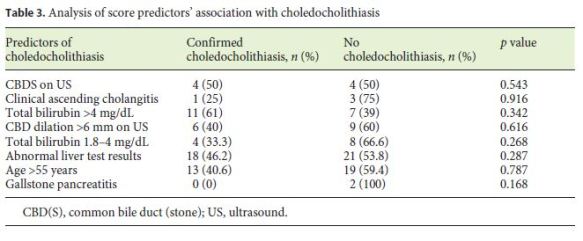
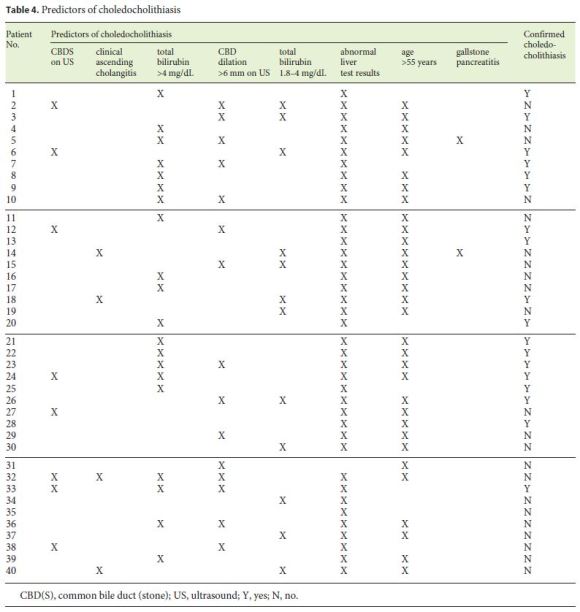
There was no significant statistical association between any of the single score predictors and the presence of choledocholithiasis (Table 3). The baseline predictors for each patient are presented in Table 4.
According to Cottons grading system for major complications of ERCP and endoscopic sphincterotomy [8], there was 1 mild complication, bleeding after ERCP, which was controlled with an adrenalin injection. The complication rate was 3.6% (1/28). None of the patients had post-ERCP pancreatitis, perforation, or infection.
Discussion
In our series, suspicion of choledocholithiasis in patients with acute cholecystitis was a rare event (<1%), which supports the findings of some authors [3]. None of the patients of the present series was readmitted because of suspected choledocholithiasis (median follow-up of 29 months).
While the sensitivity of the high risk score was approximately the same as found in published series in patients with suspected choledocholithiasis overall (86%), the positive predictive value was significantly lower (52 vs. 71–79%) [9–12]. A similar finding was made for the intermediate risk score, where both the sensitivity and positive predictive value in our series were lower than those described in published series on patients with suspected choledocholithiasis (14.4 and 41%, respectively) [9–12].
This translates into a high number of false positives and a high rate of unnecessary ERCPs (39.3%; n = 11), especially among patients with a high probability score of choledocholithiasis (10 patients with HLC and 1 patient with ILC). As ERCP is an invasive procedure with significant morbidity and mortality [13], we propose that in these patients we perform a diagnostic examination to confirm the suspicion of choledocholithiasis, such as MRCP or EUS, prior to ERCP.
MRCP is a noninvasive test with a high sensitivity and specificity for the detection of choledocholithiasis (92 and 97%, respectively) [14] – comparable with the accuracy of ERCP and IOC – which should be more frequently used in these patients. Recent studies have even suggested the systematic use of MRCP in patients with acute cholecystitis to exclude CBDS [1, 15, 16]. Another option is EUS, an invasive test with a sensitivity of 93% and a specificity of 96% for detection of choledocholithiasis [14] but with a lower morbidity than ERCP. EUS also has the advantage of performing ERCP in positive cases immediately after EUS, in the same anesthetic procedure. In the future, it would be interesting to compare the diagnostic performance of MRCP and EUS in patients presenting with acute cholecystitis.
We did not study the group of patients without any suspicion of choledocholithiasis, and this is the main limitation of our study – although we posit that the presence of clinically relevant CBDS in those patients is highly unlikely, as none of them was readmitted with symptomatic choledocholithiasis. Other limitations are the smallness of the sample of patients included in the analysis, and the fact that it was a retrospective study. However, considering the low estimated incidence of choledocholithiasis in this setting, it would take a prospective sample of several thousand patients with acute cholecystitis in order to have an adequately powered study. Another limitation is the high rate of failed cannulations, mainly due to an altered anatomy, which might have influenced the results. Finally, the diagnosis of acute cholecystitis was based on encoded information, which has some limitations such as the possibility of misdiagnosis or the lack of objectivity regarding the diagnostic criteria.
Since in the diagnosis of choledocholithiasis in this particular type of patients the clinical relevance of a test relies on its ability to identify patients with the disease (the positive predictive value), we conclude from this study that the choledocholithiasis score is not suitable for use in patients with acute cholecystitis and elevated bilirubin levels.
Conclusions
In our series, the ASGE choledocholithiasis score was not useful for diagnosing CBDS in patients presenting with acute cholecystitis. Therefore, in patients with acute cholecystitis and suspected choledocholithiasis, this score should not be used to diagnose CBDS, and another diagnostic method, such as EUS or MRCP, should be employed prior to ERCP.
References
1 Nebiker CA, Baierlein SA, Beck S, von Flue M, Ackermann C, Peterli R: Is routine MR cholangiopancreatography(MRCP) justified prior to cholecystectomy? Langenbecks Arch Surg 2009;394:1005–1010. [ Links ]
2 Peng WK, Sheikh Z, Nixon SJ, Paterson- Brown S: Role of laparoscopic cholecystectomy in the early management of acute gallbladder disease. Br J Surg 2005;92:586–591. [ Links ]
3 Videhult P, Sandblom G, Rudberg C, Rasmussen IC: Are liver function tests, pancreatitis and cholecystitis predictors of common bile duct stones? Results of a prospective, population-based, cohort study of 1,171 patients undergoing cholecystectomy. HPB (Oxford) 2011;13:519–527. [ Links ]
4 Chang CW, Chang WH, Lin CC, Chu CH, Wang TE, Shih SC: Acute transient hepatocellular injury in cholelithiasis and cholecystitis without evidence of choledocholithiasis. World J Gastroenterol 2009;15:3788–3792. [ Links ]
5 Stott MA, Farrands PA, Guyer PB, Dewbury KC, Browning JJ, Sutton R: Ultrasound of the common bile duct in patients undergoing cholecystectomy. J Clin Ultrasound 1991;19:73–76. [ Links ]
6 Costi R, Sarli L, Caruso G, Iusco D, Gobbi S, Violi V, Roncoroni L: Preoperative ultrasonographic assessment of the number and size of gallbladder stones: is it a useful predictor of asymptomatic choledochal lithiasis? J Ultrasound Med 2002;21:971–976. [ Links ]
7 ASGE Standards of Practice Committee, Maple JT, Ben-Menachem T, Anderson MA, Appalaneni V, Banerjee S, Cash BD, Fisher L, Harrison ME, Fanelli RD, Fukami N, Ikenberry SO, Jain R, Khan K, Krinsky ML, Strohmeyer L, Dominitz JA: The role of endoscopy in the evaluation of suspected choledocholithiasis. Gastrointest Endosc 2010;71:1–9. [ Links ]
8 Cotton P, Vennes J, Russel R, Liguory C: Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc 2992;37:383–393. [ Links ]
9 Narvaez Rivera RM, Gonzalez Gonzalez JA, Monreal Robles R, Garcia Compean D, Paz Delgadillo J, Garza Galindo AA, Maldonado Garza HJ: Accuracy of ASGE criteria for the prediction of choledocholithiasis. Rev Esp Enferm Dig 2016;108:309–314. [ Links ]
10 Adams M, Hosmer AE, Wamsteker EJ, Anderson MA, Elta GH, Kubiliun NM, Kwon RS, Piraka CR, Scheiman JM, Waljee AK, Hussain HK, Elmunzer BJ: Predicting the likelihood of a persistent bile duct stone in patients with suspected choledocholithiasis: accuracy of existing guidelines and the impact of laboratory trends. Gastrointest Endosc 2015;82:88–93. [ Links ]
11 Rubin M, Thosani N, Tanikella R, Wolf SD, Fallon BM, Lukens JF: Endoscopic retrograde cholangiopancreatography for suspected choledocholithiasis: testing the current guidelines. Dig Liver Dis 2013;45:744–749. [ Links ]
12 Magalhães J, Rosa B, Cotter J: Endoscopic retrograde cholangiopancreatography for suspected choledocholithiasis: from guidelines to clinical practice. World J Gastrointest Endosc 2015;7:128–134. [ Links ]
13 Andriulli A, Loperfido S, Napolitano G, Niro G, Valvano MR, Spirito F, Pilotto A, Forlano R: Incidence rates of post-ERCP complications: a systematic survey of prospective studies. Am J Gastroenterol 2007;102:1781–1788. [ Links ]
14 Verma D, Kapadia A, Eisen GM, Adler DG: EUS versus MRCP for detection of choledocholithiasis. Gastrointest Endosc 2006;64:248–254. [ Links ]
15 Wong H, Chiu Y, Shiu B, Ho L: Preoperative MRCP to detect choledocholithiasis in acute calculous cholecystitis. J Hepatobiliary Pancreat Sci 2012;19:458–464. [ Links ]
16 Tonolini M, Ravelli A, Villa C, Bianco R: Urgent MRI with MR cholangiopancreatography (MRCP) of acute cholecystitis and related complications: diagnostic role and spectrum of imaging findings. Emerg Radiol 2012;19:341–348. [ Links ]
Statement of Ethics
This study did require neither informed consent nor review/approval by the appropriate ethics committee.
Disclosure Statement
The authors declare no conflicts of interest.
* Corresponding author.
Dr. Catarina Gouveia
Serviço de Gastrenterologia, Hospital Beatriz Ângelo
Rua Melvin Jones, n°6, 2°B
PT–1600-867 Lisbon (Portugal)
E-Mail catarinagouveia228@gmail.com
Received: November 16, 2016; Accepted after revision: July 4, 2017

