










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.25 no.2 Lisboa abr. 2018
https://doi.org/10.1159/000478987
ENDOSCOPIC SNAPSHOT
Ligate-and-Resect Technique for Resection of a Large Pseudo-Pedunculated Subepithelial Lesion in the Ascending Colon
Técnica de ligadura e resseção para a exérese de uma lesão pseudo-pediculada volumosa no cólon ascendente
Sofia Silva Mendesa–c, Rolando Pinhob, Sónia Leiteb, Ana Ponteb, Joana Silvab, Jaime Rodriguesb, Mafalda Sousab, João Carvalhob
aDepartment of Gastroenterology, Braga Hospital, Braga, bDepartment of Gastroenterology, Centro Hospitalar de Vila Nova de Gaia/Espinho, Vila Nova de Gaia, and cLife and Health Sciences Research Institute (ICVS), School of Medicine, University of Minho, Braga, Portugal
* Corresponding author.
Keywords: Lipoma, Colon, Polypectomy
Palavras-Chave: Lipoma, Cólon, Polipectomia
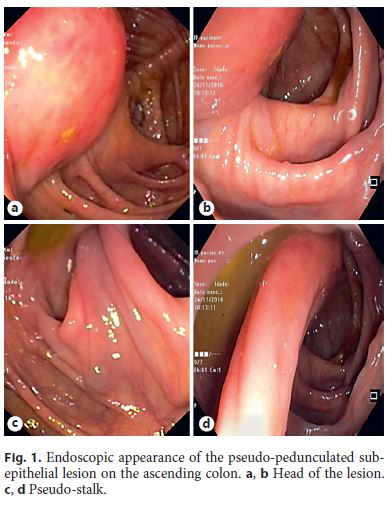
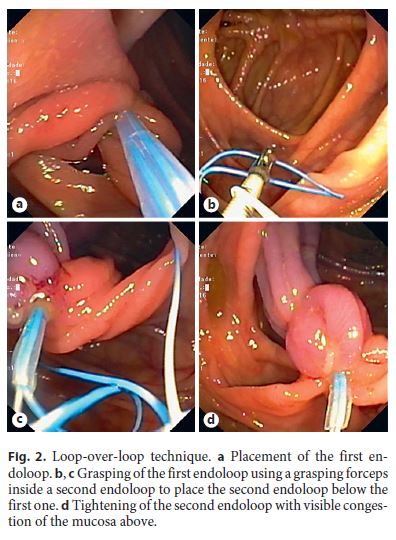
A 66-year-old male with a medical history of diabetes and hypertension was referred for resection of a large pedunculated lesion in the ascending colon, found in a screening colonoscopy. During the second colonoscopy, a pseudo-pedunculated subepithelial lesion with 35 mm (Fig. 1a, b) and a long and thick pseudo-stalk (Fig. 1c, d) was found in the ascending colon. The mucosa over the lesion was congestive with discrete erosions and a slight yellow tone from the subepithelial lesion was evident. With a dual channel colonoscope (Olympus, CF-2T160I), an endoloop (Olympus, MAJ-254) was placed near the base of the pseudo-stalk (Fig. 2a). Using the loop-over-loop technique, a second endoloop was placed below the first endoloop (Fig. 2b). A grasping forceps placed in the second working channel was used to pull the first endoloop and retract the lesion into the second endoloop (Fig. 2c, d). Resection of the lesion with a conventional oval snare was then safely performed above the two endoloops (Fig. 3a, b) and the lesion was captured (Fig. 3c, d) for histological analysis, which revealed complete resection of a 30-mm lipoma with non-dysplastic overlying mucosa.

Colonic lipomas are benign adipose tissue tumors predominantly arising from the submucosal layer, with a reported incidence of approximately 0.2–4.4% [1]. In most cases, colonic lipomas are asymptomatic and found incidentally [1]. Nevertheless, large lipomas (>20 mm) are more prone to cause abdominal pain, diarrhea, or constipation, and less frequently, gastrointestinal bleeding, intestinal occlusion, and intussusception [1]. In this case, the lipoma was felt prone to complications as it was large and very mobile from its pseudo-pedunculated morphology and already had an overlying congestive and eroded mucosa resulting from mechanical trauma from peristalsis. As there is no consensus on the resection or surveillance of asymptomatic large colonic lipomas, the patient must be involved in the decision. Resection is usually the preferred option because of the fear of complications and the relative low risk of the endoscopic techniques when the characteristics of the lesion are favorable, as in this case [1]. One of the most common practices for the treatment of large subepithelial colonic lipomas is the ligate-and-let-go technique along with removal of one fragment of the lesion for histological analysis using the unroofing technique [2–4]. The use of two endoloops increases the efficacy of this technique and reduces the risk of perforation [5]. In this case, the long pseudo-stalk allowed the safe resection of the lesion after placement of the two endoloops, with the advantages of histological characterization of the entire lesion and higher complete resection rate. Thus, in selected cases, this approach may be an alternative to consider to the ligate-and-let-go technique.
References
1 Nallamothu G, Adler DG: Large colonic lipomas. Gastroenterol Hepatol 2011;7:490–492. [ Links ]
2 Ponte A, Pinho R, Rodrigues A, Vale S, Cidade C, Silva J, Rodrigues J, Sousa M, Carvalho J: Endoscopic resection of large gastrointestinal lipomas: loop-and-let-go technique with some twists. Gastroenterol Hepatol 2016;pii:S0210-5705(16)30063-2. [ Links ]
3 Veloso R, Pinho R, Rodrigues A, Pais T, Fernandes C, Carvalho J, Fraga J: Endoloop ligation (loop-and-let-go) of a large ileal lipoma by balloon-assisted enteroscopy. Endoscopy 2012;44:176. [ Links ]
4 Ponte A, Pinho R, Vale S, Fernandes C, Ribeiro I, Silva J, Carvalho J: Resection of a large ileal lipoma exhibiting ball-valve prolapse into the cecum with a grasp-to-retract, ligate, unroof, and let-go technique. Endoscopy 2015;47:E215–E216. [ Links ]
5 Lee SH, Park JH, Park DH, Chung IK, Kim HS, Park SH, Kim SJ, Cho HD: Endoloop ligation of large pedunculated submucosal tumors (with videos). Gastrointest Endosc 2008;67:556–560. [ Links ]
Statement of Ethics
This study did not require informed consent nor review/approval by the appropriate ethics committee.
Disclosure Statement
The authors declare no conflicts of interest.
* Corresponding author.
Dr. Sofia Silva Mendes
Department of Gastroenterology, Braga Hospital
Rua das Sete Fontes
PT–4710-243 Braga (Portugal)
E-Mail sofiadasilvamendes@gmail.com
Received: January 6, 2017; Accepted after revision: June 20, 2017

