










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.25 no.3 Lisboa jun. 2018
https://doi.org/10.1159/000484251
ENDOSCOPIC SNAPSHOT
Stenosis of Hepaticojejunal Anastomosis with Intrahepatic Lithiasis: Treatment with Single-Balloon Enteroscopy-Assisted ERCP
Estenose de Anastomose Hepatico-Jejunal com Litíase Intra-Hepática: Tratamento por CPRE Assistida por Enteroscópio de Mono-Balão
Jaime P. Rodrigues, Rolando Pinho, Luísa Proença, Joana Silva, Ana Ponte, Mafalda Sousa, João Carlos Silva, João Carvalho
Gastroenterology Department, Centro Hospitalar Vila Nova de Gaia/Espinho, Vila Nova de Gaia, Portugal
* Corresponding author.
Keywords: ERCP, Enteroscopy, Stricture, Dilation
Palavras-Chave: CPRE, Enteroscopia, Estenose, Dilatação
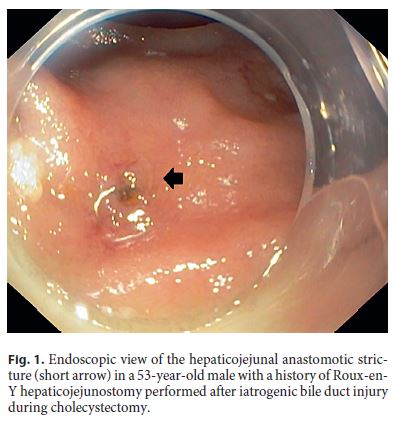
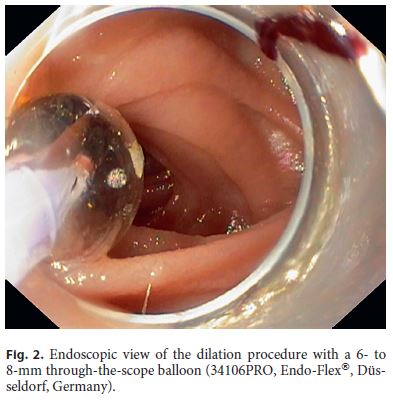
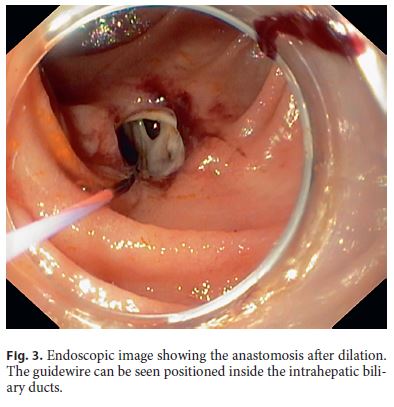
A 53-year-old male patient with a history of Roux-en-Y hepaticojejunostomy due to an iatrogenic lesion of the biliary tract during cholecystectomy in 2013 presented with recurrent episodes of acute cholangitis. Magnetic resonance cholangiopancreatography showed dilation of the intrahepatic biliary ducts associated with intrahepatic lithiasis. Due to a high index of suspicion of hepaticojejunal anastomosis stenosis not evident in the magnetic resonance cholangiopancreatography, the patient was referred to our department for enteroscopy-assisted endoscopic retrograde cholangiopancreatography (ERCP). The procedure was performed with a single-balloon enteroscope (SIF-Q180, Olympus Medical Systems®, Tokyo, Japan) with a transparent cap attached at its tip. After identification of the Roux-en-Y anastomosis, the afferent limb was intubated, followed by progression to the hepaticojejunal anastomosis. A severe stricture of the anastomosis was identified (Fig. 1). A 0.035-inch guidewire (METII-35-600E, Tracer Metro® DirectTM Wire Guide, Cook®, Bloomington, IN, USA) was passed through the stricture followed by a sphincterotome (CCPT-25ME, Classic Cotton® CannulaTome®, Cook®). Upon contrast injection, dilation of the intrahepatic ducts was evident. Dilation with a 6- to 8-mm through-the-scope balloon (34106PRO, Endo-Flex®, Düsseldorf, Germany) was then performed (Fig. 2, 3) with immediate spontaneous drainage of multiple small calculi. The intrahepatic bile ducts were explored with a balloon catheter, but no more calculi were identified. The patient was discharged on the second day after the procedure and did not present additional episodes of acute cholangitis after a 6-month follow-up.
ERCP is an essential therapeutic technique for a wide range of pancreatobiliary conditions and presents a 90– 95% success rate in patients with native gastric and pancreaticoduodenal anatomy [1]. In Roux-en-Y surgical reconstruction (hepaticojejunostomy and choledochojejunostomy, gastric bypass surgery, or post-Whipple surgery), ERCP is often unsuccessful because of the inability to reach the anastomosis [1]. Double-balloon enteroscopy was initially introduced as a useful procedure to access surgically excluded intestinal segments [2]. Posteriorly, single-balloon enteroscope, an alternative method for small-bowel evaluation, proved to be safe and useful for engaging in biliary endotherapy [1, 3, 4]. However, the technique presents several limitations, namely the frontal view of the enteroscope (as opposed to the lateral view of conventional duodenoscopes), the smaller caliber channel, and the longer channel length [5]. Moreover, available standard ERCP accessories cannot be used with the enteroscope [5]. These limitations turn the procedure challenging and more demanding than standard ERCP. The use of a cap attached to the distal tip of the enteroscope can improve the endoscopic position and add stability for biliary cannulation. In consequence, and in contrast to patients with native anatomy, in patients with hepaticojejunal anastomosis the cannulation success rate is approximately 70% [1].
This case illustrates the gradual improvement of endoscopic biliary interventions in patients with surgically altered anatomy. With the development of device-assisted ERCP, access to the pancreatic and biliary duct systems in patients with surgically altered anatomies is now possible, although technically challenging and time consuming.
References
1 Saleem A, Baron TH, Gostout CJ, et al: Endoscopic retrograde cholangiopancreatography using a single-balloon enteroscope in patients with altered Roux-en-Y anatomy. Endoscopy 2010;42:656–660. [ Links ]
2 Sakakihara I, Kato H, Muro S, et al: Double-balloon enteroscopy for choledochojejunal anastomotic stenosis after hepato-biliary-pancreatic operation. Dig Endosc 2015;27:146–154. [ Links ]
3 Pinto-Pais T, Pinho R, Proença L, et al: Iatrogenic biliary injury in a patient with Roux-en- Y hepaticojejunostomy: stenting repair with single-balloon enteroscopy-assisted ERCP. Endoscopy 2014; 46:E506–E507. [ Links ]
4 Wang AY, Sauer BG, Behm BW, et al: Single-balloon enteroscopy effectively enables diagnostic and therapeutic retrograde cholangiography in patients with surgically altered anatomy. Gastrointest Endosc 2010;71:641– 649. [ Links ]
5 Pinho R, Proença L, Alberto L, et al: Biliary self-expandable metallic stent using single balloon enteroscopy assisted ERCP – overcoming limitations of current accessories. Rev Esp Enferm Dig 2013;105:561–564. [ Links ]
Disclosure Statement
The authors do not have any interest which might be interpreted as influential in this report. This report did not receive any support from corporations, industrial or private.
* Corresponding author.
Dr. Jaime P. Rodrigues
Gastroenterology Department, Centro Hospitalar Vila Nova de Gaia/Espinho
Rua Conceição Fernandes
PT–4434-502 Vila Nova de Gaia (Portugal)
E-Mail jaimepereirarodrigues@gmail.com
Received: April 27, 2017; Accepted after revision: August 9, 2017

