










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.25 no.5 Lisboa out. 2018
https://doi.org/10.1159/000485428
ORIGINAL ARTICLE
Intragastric Balloon for Obesity Treatment: Safety, Tolerance, and Efficacy
Balão Intragástrico no Tratamento da Obesidade: Segurança, Tolerância e Eficácia
Joana Ribeiro da Silva, Luísa Proença, Adélia Rodrigues, Rolando Pinho, Ana Ponte, Jaime Rodrigues, Mafalda Sousa, Rita Almeida, João Carvalho
Department of Gastroenterology, Centro Hospitalar Vila Nova de Gaia/Espinho, Vila Nova de Gaia, Portugal
* Corresponding author.
ABSTRACT
Background: Obesity is an increasing worldwide problem associated with a vast number of comorbidities. Decreasing body weight by only 5–10% has been shown to slow and even prevent the onset of obesity-related comorbidities. Between pharmacological therapy and bariatric surgery a great variety of endoscopic techniques are available, the most common being intragastric balloon (IGB). The purpose of this study was to assess the safety, tolerance, and kinetics of IGBs in weight loss. The kinetics of weight loss were evaluated in 2 different contexts and phases: after the IGBs removal and after follow-up that varied between 6 and 12 months. Successful weight loss was defined as ≥10% weight loss after 6–12 months. Methods: The study included 51 patients who had undergone Orbera® IGB placement between September 2014 and February 2016. Inclusion criteria were age between 18 and 65 years; body mass index (BMI) 28–35 with severe obesity-related disorders; or BMI 35–40. The IGB was removed 6 months later. All patients were followed for a minimum period of 6–12 months. Results: Of 51 patients, 16 were excluded (7 due to intolerance) and 35 patients entered the study, of which 83% were followed for more than 6–12 months. The average weight loss (WL) and % excess WL (%EWL) after 6 months of treatment were 11.94 kg and 42.16%, respectively. At 6–12 months, after removal of the IGB, the mean WL was 8.25 kg and %EWL was 30.27%. Nineteen patients attained a WL of ≥10% the baseline value at IGB removal and 12 maintained their weight below this threshold during the 6–12 following months. Conclusions: After temporary IGB implantation in overweight or obese individuals, a WL that was ≥10% of weight at baseline was achieved in 54.3% and sustained at 6–12 months in 41.4% of participants. IGBs are an attractive intermediate option between diet and exercise programs and bariatric surgery. In general, IGB placement is a safe and well-tolerated procedure.
Keywords: Intragastric balloon, Obesity treatment, Orbera® intragastric balloon
RESUMO
Introdução: A obesidade, problema crescente, está associada a um grande número de comorbilidades. A redução do peso corporal em apenas 5–10% mostrou-se eficaz na melhoria e até na prevenção do aparecimento de comorbilidades relacionadas com a obesidade. Entre a terapia farmacológica e a cirurgia bariátrica, temos disponíveis uma grande variedade de técnicas endoscópicas, sendo a mais comum a colocação de balão intragástrico (BIG). O objectivo do estudo foi avaliar a segurança, tolerância e cinética da perda de peso do BIG. A cinética da perda de peso foi avaliada em dois momentos e contextos distintos: após a remoção do balão e depois do periódo de follow-up (PFU), que variou entre 6–12 meses. Eficácia definida como perda de peso 10% após PFU de 6–12 meses. Métodos: O estudo incluiu 51 pacientes que colocaram Orbera® BIG entre setembro de 2014 e fevereiro de 2016. Os critérios de inclusão foram: idade entre 18–65 anos, IMC 28–35 com comorbilidades relacionadas com obesidade e IMC 35–40. O BIG foi removido passados 6 meses. Todos os doentes foram acompanhados por um período minino de 6–12 meses (PFU). Resultados: Dos 51 doentes considerados, 16 foram excluidos (7 por intolerancia) e 35 entraram no estudo, dos quais 83% foram seguidos durante PFU. A perda de peso média (PPM) e % de excesso de peso perdido (EPP) na altura de remoção do BIG foi de 11.94 kg e 42.16%, respetivamente; após PFU, a PPM foi de 8.25 kg e o EPP foi 30.27%. Dezanove alcançaram uma perda de peso na altura de remoção de BIG e 12 mantiveram o seu peso abaixo deste limiar após o PFU. Conclusões: Após a colocação temporaria do BIG em pacientes com excesso de peso ou obesidade, foi alcançado uma perda de peso superior a 10 em 54.3% na altura de remoção do BIG e sustentada após periodo de follow-up de 6–12 meses em 41.4% dos doentes. Os BIG são uma alternativa intermédia atractiva entre dieta/exercicio fisico e cirurgia bariátrica. Em geral é um procedimento seguro e bem tolerado.
Palavras-Chave: Balão intragástrico, Tratamento da obesidade, Orbera®
Introduction
Obesity is an increasing worldwide problem with devastating health consequences [1]. Worldwide, more than 1.4 billion adults are overweight or obese and face an increased risk of numerous, potentially disabling conditions [2]. Obesity is associated with a vast number of comorbidities, including coronary heart disease, type 2 diabetes mellitus, stroke, sleep apnea, musculoskeletal disease, and an increase in the prevalence of certain cancers [3].
The health benefits of weight reduction are well established. Decreasing body weight by only 5–10% has been shown to slow and even prevent the onset of obesity-related comorbidities [4, 5]. However, permanent weight loss is frequently difficult to achieve [6], and the availability of safe and effective weight loss therapies is limited [2]. The conventional treatments, such as a calorie-restricted diet, regular physical activity, and behavioral modification, are frustrating procedures which take a long time before any significant result can be observed [7, 8].
Pharmacological therapy is indicated for patients with a body mass index (BMI) ≥30 or ≥27 if obesity-related risk factors or diseases are present [5]. Pharmacotherapy is less invasive and less costly for the management of obesity but results in a limited weight loss and may have significant side effects [9].
Bariatric surgery is the most effective weight loss intervention [10], resulting in long-term sustained weight loss [10] and long-term resolution of comorbidities [11]. It is, however, restricted to patients with morbid obesity (BMI >40) [12]. Despite all of its advantages, bariatric surgery is still extremely invasive and costly and is likely to cause a vast number of complications that may prove to be fatal [13]. However, there is an intermediate group of patients who do not respond to medical therapy and who do not qualify for the bariatric procedure.
In recent years, new endoscopic techniques have emerged, thus providing less invasive and more cost-effective options for the treatment of obesity. Endoscopic modalities in the treatment of obesity can be categorized into the following: space-occupying devices (intragastric balloon [IGB], transpyloric shuttle), gastric restrictive methods (transoral gastroplasty, transoral endoscopic restrictive implant system), malabsorptive endoscopic procedures (duodenal-jejunal bypass liner, satiSphere), regulating gastric emptying (intragastric botulinum toxin injections, gastric electrical stimulation), and other therapies (aspiration therapy) [14–16]. Of these methods, the most commonly employed is IGB placement.
The first generation of IGBs date back to 1985 [2]. These balloons, filled with 220 mL of air, were endoscopically placed and left in the stomach for 3 months, then being removed endoscopically. This procedure was withdrawn from the market, not only because of severe procedure-related complications but also due to lack of efficacy. Since then, different balloons have been tested, resulting only in short-term results or being associated with technical problems [2].
Safer and more effective IGBs were subsequently developed over the next 2 decades that were more effective at promoting weight loss [2]. Nowadays, the most commonly used IGB worldwide is the Orbera® IGB (formerly the Bioenterics IGB). These balloons, which are filled with saline solution, are placed endoscopically in the stomach, remaining there for 6 months, and are then removed in a subsequent endoscopy. The IGB decreases preprandial hunger, increases postprandial satiety, and promotes weight loss in the short term [12].
The IGB is an attractive intermediate option between prescription drugs and bariatric surgery for overweight and obese patients hoping to lose a significant amount of weight without the invasiveness of surgery or the systemic side effects of pharmacotherapy. The minimal invasiveness and temporary nature of the IGB is attractive, but the duration of implantation, during which the patient is closely followed, is short. Whether this shortterm follow-up is sufficient to change the patients lifestyle and eating practices and to maintain their weight reduction after IGB removal is still a subject of controversy [17].
We have prospectively followed a cohort of patients treated with the IGB to induce weight loss. The aim of this study was to assess the safety, tolerance, and kinetics of weight loss during and after IGB therapy, with a minimum follow-up of 6 months after IGB implantation. On the other hand, we sought to evaluate changes in the metabolic parameters associated with weight reduction.
Materials and Methods
Patients and Design of the Study
A prospective single-center study was conducted on 51 patients who had undergone the Orbera® IGB procedure between September 2014 and February 2016. All patients were screened for major endocrine disorders before admission to the study. All procedureswere performed by 2 of the authors, who have extensive experience in IGB therapy. Informed consent was obtained from all patients before the procedure.
Inclusion criteria were the following: (1) age between 18 and 65 years; (2) BMI >28 and <35 with severe obesity-related disorders who had failed to achieve weight loss with an adequate weight loss program for 3 years; (3) BMI ≥35 and ≤40. Exclusion criteria were a history of malignancy within the previous 5 years, previous bariatric or gastrointestinal surgery, alcohol or drug abuse, hormonal or genetic causes of obesity, women referred from the infertility clinic, use of anticoagulants or nonsteroidal anti-inflammatory drugs, pregnancy, gastric or esophageal varices, large hiatus hernia (>5 cm in length), reflux esophagitis grade C or D on the Los Angeles classification, duodenal or gastric ulcer, and other lesions considered to be high risk for bleeding.
Procedure
The IGB was placed with the patient under anaesthesiologist-administered propofol sedation. A complete upper gastrointestinal endoscopy was previously performed to exclude abnormalities. The balloon was inserted blindly into the gastric body collapsed within a specially designed sheath, as presented in the commercially available pack. Then, the endoscope was reinserted, and the balloon was inflated under direct endoscopic vision with saline (600 mL) and methylene blue (5 mL) solution. After the procedure, the patients were kept in the recovery room for 2 h for observation and for symptom control. Once they could tolerate a liquid diet, they were discharged medicated with proton pump inhibitors, which they were indicated to maintain until removal of the IGB, and with antiemetic agents for 1 week.
The patients were advised to follow a fully liquid diet for the first 4 weeks, and a soft diet was gradually introduced thereafter. During the 6 months of treatment, a balanced diet with 1,100 kcal/ day and 20% protein was prescribed by the nutritionist to all patients (regardless of the BMI).
Patients were followed twice a week for the first week, then at the end of the first month, and finally at 3 and 6 months. During the follow-up visits with the nutritionist, the nutrition plan and the weight control were evaluated, and nutritional education was reinforced.
The IGB was removed 6 months later under endoscopic control using the IGB removal kit. Then, all patients were followed on an outpatient basis by the nutritionist for a period of 6–12 months after placement of the IGB.
Parameters
The patients underwent complete physical examination, anthropometry (body weight, BMI, percentage of body weight loss, and fat mass), blood pressure measurement, and determination of serum triglycerides, high-density lipoprotein (HDL) and low-densitylipoprotein (LDL) cholesterol, glucose, and liver enzymes (ALT, GGT) at baseline, 6 months (time of IGB removal), and 6–12 months after IGB removal.
The Anthropometric evaluation was performed using bioimpedance(Tanita TBF-300®). Successful weight loss was defined as ≥10% weight loss after 6–12 months.
Statistical Analysis
Discrete variables are presented as proportions, and continuous variables are presented using the mean and standard distribution. The normal distribution of continuous variables was confirmed using the Kolmogorov-Smirnov test. Continuous variables were compared across 2 time periods using the paired-samples t test. Results were considered as statistically significant if p < 0.05.The Statistical Package for the Social Sciences (SPSS 20.0) was used for data entry and data analysis.
Results
Sample Characteristics
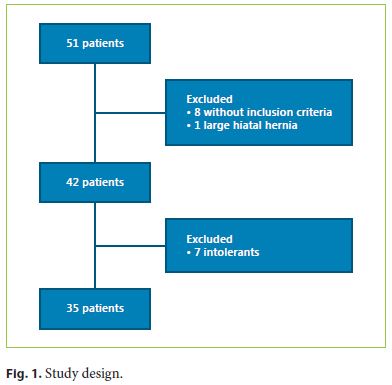
The IGB was placed in 51 consecutive patients between September 2014 and February 2016. Of these 51 patients, 8 did not meet the inclusion criteria and 1 was excluded before the placement of the IGB due to a large hiatal hernia. Considering the 42 patients who received the IGB, 7 did not tolerate it (Fig. 1). In total, 35 patients entered the study, of which 29 (83%) were followed for more than 6–12 months.
The baseline characteristics are presented in Table 1. All 35 patients completed a 6-month period with the IGB, 31 of which were female and 4 male. The mean age was 41.3 ± 9.6 years; the mean weight was 94.6 ± 11.9 kg, the mean BMI was 35.8 ± 4.0, and the mean initial excess weight was 28.7 ± 8.9 kg.
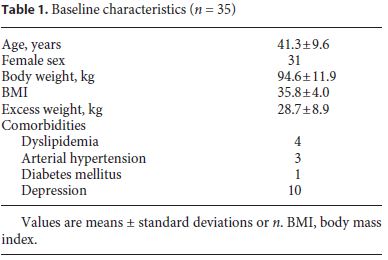
Regarding comorbidities, 8.6% of the patients suffered from arterial hypertension, 11.4% from hyperlipidemia, 2.8% from diabetes, and 28.6% from chronic depression. During the examination, we observed 1 case with esophagitis and 1 case with peptic ulcers.
All endoscopic placements were successfully performed in 10 ± 4 min, and 600 mL of saline were injected in every patient. There were no serious complications, except for nausea and vomiting, and the average recovery period was 2 ± 1 h.
IGB Removal
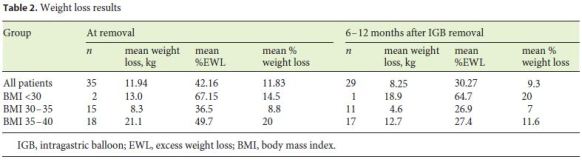
The average weight loss and % excess weight loss (%EWL) after 6 months of treatment were 11.94 kg and 42.16%, respectively. Upon IGB removal, in patients with a baseline BMI <30 (n = 2), the mean weight loss was 13 kg and the mean %EWL was 67.15%; in patients with a baseline BMI 30–35 (n = 15), the mean weight loss was 8.3 kg and the mean %EWL was 36.5%; in patients with a baseline BMI 35–40 (n = 18), the mean weight loss was 21.1 kg and the mean %EWL was 49.7% (Table 2).
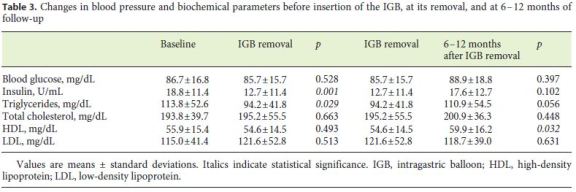
Compared to baseline values, the patients experienced significant reductions in weight (93.8 ± 11.0 to 81.9 ± 10.4 kg, p < 0.001), BMI (35.8 ± 3.9 to 31.8 ± 2.6, p < 0.001), and fat mass (42.7 ± 7.1 to 31.8 ± 7.4 kg, p < 0.001). Compared to baseline values, a significant improvement in triglyceride level and insulin, but not in HDL cholesterol, total cholesterol, LDL cholesterol, and glucose levels, was seen (Table 3).
Follow-Up after IGB Removal
Patients who completed 6–12 months of follow-up after IGB removal followed no structured weight maintenance program, and they attended 1 visit with a nutritionist. Six patients were lost to follow-up. At 6–12 months after removal of the IGB, the mean weight loss was 8.25 kg and the mean %EWL was 30.27% for the group as a whole; 18.9 kg and 64.7% for patients with a BMI <30 (n = 1); 4.6 kg and 26.9% for patients with a BMI 30–35 (n = 11); and 12.7 kg and 27.4% for patients with a BMI 35–40 (n = 17), respectively (Table 2). Compared to baseline values, patients showed significant reductions in weight (93.8 ± 11.0 to 86.9 ± 13.4 kg, p < 0.001), BMI (35.8 ± 3.9 to 33.5 ± 4.3, p < 0.001), and fat mass (42.7 ± 7.1 to 36.2 ± 9.9 kg, p < 0.001).
Regarding weight loss results, a generally accepted criterion used in clinical treatments was used: the method has failed if %EWL is <20%. According to this criterion, we compared %EWL at 2 time points (Table 4): immediately after IGB removal and 6–12 months later. Just after
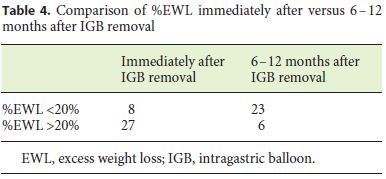
IGB removal, there were 8 patients with a %EWL <20% (unsatisfactory results) and 27 patients with a %EWL >20% (good results). At 6–12 months after the IGB had been removed, there were 23 patients with a %EWL <20% (unsatisfactory results) and 6 patients with a %EWL >20% (good results). On the other hand, 19 patients attained a weight loss of ≥10% the baseline value at IGB removal and 12 maintained their weight below this threshold during the 6–12 following months, while 7 regained weight above this threshold. Compared to IGB removal values, a significant improvement in HDL cholesterol, but not in insulin, triglycerides, total cholesterol, LDL cholesterol, and glucose levels, was seen (Table 3).
Complications
Complications were observed in 7 patients. These consisted of abdominal pain, nausea, and vomiting (food intolerance, n = 5) and spontaneous IGB deflation (n = 1). All complications resolved with IGB removal, either unexpectedly through vomiting after spontaneous deflation (n = 1) or endoscopic extraction (n = 6). Additionally, unexpected pregnancy led to the extraction of 1 IGB at 3.7 months after implantation (without complications at birth). Gastroscopy during the removal procedure was normal in 32 patients and revealed esophagitis in 1 patient and peptic ulcers in 2 patients.
Discussion
Earlier generations of IGBs had a limited volume (200–220 mL), were filled with air, had a low resistance to gastric acid, and the treatments lasted a maximum of 3–4 months. This may explain spontaneous balloon deflation, passage of the balloon through the digestive tract, and insufficient weight loss with air-filled IGBs. Current-generation balloons have an intragastric capacity of up to 960 mL, are filled with saline solution, and have fewer adverse effects.
IGBs affect both the stretch receptors and the gastric capacity and increase satiety while decreasing the residual volume available for food and, therefore, could be considered a nonsurgical restrictive procedure to treat obesity. Compared with surgical treatment, the IGB can be attractive for patients. This treatment is less invasive than surgery, can be repeated, and is completely reversible. On the other hand, this treatment is temporary, because the IGB can remain in the gastric cavity for only a limited period of time. The mean duration of IGB implantation in our series was 6 months.
The question remains whether the obese patients food practices and lifestyle can be modified sufficiently during this temporary process to cause significant weight loss. There are contrary results from studies that assess the long-term effectiveness of IGB: on the one hand, there are studies that conclude that patients may recover partial or total weight loss after the balloon has been removed; on the other hand, in other series, the results are encouraging. In these latter studies, the consistency of weight loss achieved during IGB therapy and the amount of weight loss sustained after IGB removal were surprisingly very similar. Thus, Datis et al. [5], Dogan et al. [18], Fuller et al. [19], Genco et al. [20], Herve et al. [21], Ohta et al. [22], and Sallet et al. [23] report that after extraction of the balloon, the majority of patients had achieved weight loss.
In our study, mean weight loss and %EWL 6 months after balloon placement were 11.94 kg and 42.16%, respectively. Studies evaluating patients at 6 months after removal include the following: Dogan et al. [18] noted that the mean weight loss at the time of balloon removal was 9.5 kg and 1 year after the removal 7.6 kg; Fuller et al. [19] noted a weight loss of 9.4 kg, Gaur et al. [2] noted a weight loss of 18.3 and 20.1 kg, and Sallet et al. [23] noted a weight a loss of 17.4 kg.
After 6–12 months of follow-up, our patients showed a mean weight loss of 8.25 kg, similar to other studies with the IGB: Dastis et al. [5] (7.9 kg), Dogan et al. [18] (7.6 kg), Herve et al. [21] (8.6 kg) and Ohta et al. [22] (6.4 kg). In our study, after IGB removal, there were 8 patients with %EWL <20 and 27 patients (77.1%) with %EWL >20%. At 6–12 months after the IGB had been removed, there were 23 patients with %EWL <20% and 6 patients (23%) with %EWL >20%.
Kotzampassi et al. [17] obtained better results. They demonstrated that the percentage of patients having EWL% of 20% was 83% at the time of balloon removal, 53 and 27% at 12 and 24 months, respectively, and 23% at the 60-month follow-up of 195 obese patients. On the other hand, we found that, after temporary IGB implantation in overweight or obese individuals, a weight loss that was ≥10% of weight at baseline was achieved in 54.3% and sustained at 6–12 months in 41.4% of participants.
Given the ease and reproducibility of the method, these results are encouraging, because they are at least equivalent to those reported with therapies recommended for weight loss or maintenance. In particular, dietetic counseling or behavioral therapy allows 15–30% of obese individuals to achieve ≥10% baseline weight loss at 1 year [5], compared to 65.5% at 6 months and 41.4% at 6–12 months in the present series.
Obesity plays a key role in the metabolic syndrome. Visceral fat accumulation, above all in the liver, is associated with a cluster of metabolic alterations, i.e., type 2 diabetes, hypertension, and dyslipidemia. Patients in our study experienced only metabolic effects. Stimac et al. [7] also demonstrated there that there were no significant differences in LDL and total cholesterol concentration.
The endoscopic examination performed before implantation of the IGB is of primary importance. During this examination, we observed 1 case of esophagitis, 1 peptic ulcer, and 1 large hiatal hernia. The last contraindicated the placement of an IGB.
As in other studies, there was a high incidence of nausea and vomiting in the first 3 days of balloon placement. However, the prophylactic prescription of antiemetic drugs in the first days reduced the intolerance, with only 7 patients (13.7%) demanding endoscopic removal of the IGB. The continuous use of proton pump inhibitors is mandatory, not only for the protection of the gastric mucosa and against gastroesophageal reflux, but also to protect the balloon itself from the deleterious action of hydrochloric acid.
During the IGB removal procedure, we observed 1 new case of esophagitis and 2 new peptic ulcers among the patients with a normal gastroscopy before implantation. Our study reports 1 case of balloon deflation, resolved by spontaneous IGB elimination through vomiting.
This study has some limitations. The anthropometric evaluation of the patients was limited to a bioimpedance evaluation. Other measurements which could add detail to the evaluation of body changes and to the impact of the IGB on body composition were not used.
The current generation of IGBs is an attractive intermediate option between diet and exercise programs and bariatric surgery; it is a safe and effective procedure in which about half of the patients can expect to maintain their weight after the balloon is removed. Since IGB represents a temporary nonsurgical and nonpharmaceutical treatment for obesity that is totally reversible and repeatable, it should be recommended to patients who have previously tried traditional methods of weight reduction which have failed. Careful patient follow-up is of primary importance to avoid complications and to support the efficacy of the treatment. One year of follow-up cannot be considered long-term, but these results are encouraging. Concurrent behavior modification is necessary for durable weight loss success.
References
1 James WP: The epidemiology of obesity: the size of the problem. J Intern Med 2008;263:336–352. [ Links ]
2 Gaur S, Levy S, Mathus-Vliegen L, et al: Balancing risk and reward: a critical review of the intragastric balloon for weight loss. Gastrointest Endosc 2015;81:1330–1336. [ Links ]
3 Billington CJ, Epstein LH, Goodwin NJ, et al: Overweight, obesity, and health risk. Arch Intern Med 2000;160:898–904. [ Links ]
4 Lau DC, Teoh H: Benefits of modest weight loss on the management of type 2 diabetes mellitus. Can J Diabetes 2013;37:128–134. [ Links ]
5 Dastis SN, François E, Deviere J, et al: Intragastric balloon for weight loss: results in 100 individuals followed for at least 2.5 years. Endoscopy 2009;41:575–580. [ Links ]
6 Fontaine KR, Redden DT, Wang C, et al: Years of life lost due to obesity. JAMA 2003;289:187–193. [ Links ]
7 Stimac D, Majanovic SK, Turk T, et al: Intragastric balloon treatment for obesity: results of a large single center prospective study. Obes Surg 2011;21:551–555. [ Links ]
8 Loveman E, Frampton GK, Shepherd J, et al: The clinical effectiveness and cost-effectiveness of long-term weight management schemes for adults: a systematic review. Health Technol Assess 2011;15:1–182. [ Links ]
9 Ling H, Lenz TL, Burns TL, et al: Reducing the risk of obesity: defining the role of weight loss drugs. Pharmacotherapy 2013;33:1308–1321. [ Links ]
10 Bult MJ, van Dalen T, Muller AF: Surgical treatment of obesity. Eur J Endocrinol 2008;158:135–145. [ Links ]
11 Ribaric G, Buchwald JN, McGlennon TW: Diabetes and weight in comparative studies of bariatric surgery vs conventional medical therapy: a systematic review and meta-analysis. Obes Surg 2014;24:437–455. [ Links ]
12 Mathus-Vliegen EM, Tytgat GN: Intragastric balloon for treatment-resistant obesity: safety, tolerance, and efficacy of 1-year balloon treatment followed by a 1-year balloon-free follow-up. Gastrointest Endosc 2005;61:19–27. [ Links ]
13 Goldfeder LB, Ren CJ, Gill JR: Fatal complications of bariatric surgery. Obes Surg 2005;16:1050–1056. [ Links ]
14 Behary J, Kumbhari V: Advances in the endoscopic management of obesity. Gastroenterol Res Pract 2015;2015:757821. [ Links ]
15 Kumar N: Endoscopic therapy for weight loss: gastroplasty, duodenal sleeves, intragastric balloons, and aspiration. World J Gastrointest Endosc 2015;7:847–859. [ Links ]
16 Norén E, Forssell H: Aspiration therapy for obesity: a safe and effective treatment. BMC Obes 2016;3:56. [ Links ]
17 Kotzampassi K, Grosomanidis V, Papakostas P, et al: 500 intragastric balloons: what happens 5 years thereafter? Obes Surg 2012;22:896–903. [ Links ]
18 Dogan UB, Gumurdulu Y, Akin MS, et al: Five percent weight lost in the first month of intragastric balloon treatment may be a predictor for long-term weight maintenance. Obes Surg 2013;23:892–896. [ Links ]
19 Fuller NR, Pearson S, Lau NS, et al: An intragastric balloon in the treatment of obese individuals with metabolic syndrome: a randomized controlled study. Obesity 2013;21:1561–1570. [ Links ]
20 Genco A, Cipriano M, Materia A, et al: Laparoscopic sleeve gastrectomy versus intragastric balloon: a case-control study. Surg Endosc 2009;23:1849–1853. [ Links ]
21 Herve J, Wahlen CH, Schaeken A, et al: What becomes of patients one year after the intragastric balloon has been removed? Obes Surg 2005;15:864–870. [ Links ]
22 Ohta M, Kitano S, Kai S, et al: Initial Japanese experience with intragastric balloon placement. Obes Surg 2009;19:791–795. [ Links ]
23 Sallet JA, Marchesini JB, Paiva DS, et al: Brazilian multicenter study of the intragastric balloon. Obes Surg 2004;14:991–998. [ Links ]
Statement of Ethics
Informed consent was obtained from all patients before the procedure.
Disclosure Statement
The authors have no conflicts of interest to declare.
* Corresponding author.
Dr. Joana Ribeiro da Silva
Department of Gastroenterology, Centro Hospitalar Vila Nova de Gaia/Espinho
Rua Conceição Fernandes
PT–4434-502 Vila Nova de Gaia (Portugal)
E-Mail joanasilva67@hotmail.com
Received: August 3, 2017; Accepted after revision: November 14, 2017

