










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.26 no.1 Lisboa fev. 2019
https://doi.org/10.1159/000487152
ENDOSCOPIC SNAPSHOT
Endoscopic Removal of Two Esophageal Over-The-Scope Clips with Cold Saline Solution Technique
Remoção Endoscópica Esofágica de Dois Over-the-Scope Clips Pela Técnica de Soro Frio
Marta Rochaa, Ricardo Küttner Magalhãesa, Luís Maiaa, Teresa Moreiraa, Sílvia Barriasa, Carlos Nogueirab, Isabel Pedrotoa
aDepartment of Gastroenterology, Hospital de Santo António/Centro Hospitalar do Porto, Porto, Portugal; bDepartment of Surgery, Hospital de Santo António/Centro Hospitalar do Porto, Porto, Portugal
* Corresponding author.
Keywords: Endoscopic clip removal, Endoscopy, Fistula,·Over-the-scope clip
Palavras-Chave: Remoção endoscópica de clips, Endoscopia, Fístula,·Over-the-scope clip
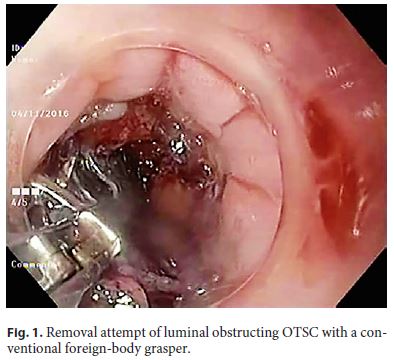
A 51-year-old man with a T4N1M0 gastric adenocarcinoma underwent neoadjuvant chemotherapy and total gastrectomy with Roux-en-Y esophagojejunostomy. Due to clinical worsening in the immediate postoperative period, an abdominal computed tomography was performed, revealing an empyema and a fistulous tract between the distal esophagus and the pleural cavity. The patient was initially treated with broad spectrum antibiotics and total parenteral nutrition, without clinical improvement. Endoscopy was then performed with identification of the esophageal orifice of the fistula and it was decided to proceed to endoscopic closure of the fistula with an over-the-scope clip (OTSC). Destruction of the epithelial lining of the accessible part of the fistulous tract with argon plasma coagulation was conducted followed by the application of an OTSC. A second OTSC was placed to ensure complete closure of the fistula. Reassessment with gastrografin transit showed no leakage of contrast. The patient resumed oral feeding with good tolerance and was discharged 10 days after the endoscopic procedure without any complications. Six weeks later he presented with dysphagia, regurgitation, and weight loss. Endoscopy documented the presence of the 2 OTSC attached to each other and partially migrated to the lumen, causing luminal obstruction at the level of the esophagojejunal anastomosis. After an unsuccessful attempt to remove them with a conventional foreign-body grasper (Fig. 1), a second attempt was performed by submerging the clips for 1 min with cold saline solution previously kept in the refrigerator (Fig. 2; online suppl. Video 1, see http://wwww.karger.com/doi/10.1159/000487152), and with successive twisting maneuvers of the corners of the OTSC with a grasper it was possible to remove them “en bloc” with little resistance (Fig. 3). Thereafter, the patient repeated a gastrografin transit with adequate contrast progression and was discharged uneventfully.


The OTSC, commonly known as the “bear claw,” can provide full-thickness closure of open defects up to 2–3 cm with greater compressive force than through-the-scope clips. Consequently, OTSC have the ability to close long-lasting leaks and fistulas even when the tissue surrounding the defect is inflamed or indurated [1]. While OTSC are able to stay in place for long periods of time, they may need to be removed under certain circumstances, as in the case of misplacement or after healing of the defect. Thus, the availability of techniques to do so is important. In the presented case, the difficulty of removal was increased by the presence of 2 OTSC attached to each other forming a conglomerate that was adherent to the mucosa. Interestingly, these clips are made of the alloy nitinol, which allows them to change stiffness based on temperature. At temperatures below 10 ° C, the material changes to its martensitic grid structure, becoming malleable and being easily capable of changing shape while applying reduced force. Once heated, the OTSC return to their original shape, generating high force [2, 3]. Thanks to this feature, the clips were removed safely.
References
1 Rogalski P, Daniluk J, Baniukiewicz A, Wroblewski E, Dabrowski A: Endoscopic management of gastrointestinal perforations, leaks and fistulas. World J Gastroenterol 2015;21:10542–10552. [ Links ]
2 Krishna SG, Shakhatreh M: Endoscopic removal of over-the-scope clip with cold saline solution technique. Gastrointest Endosc 2016;84:850–851. [ Links ]
3 Arezzo A, Bullano A, Fischer H, Morino M: The way to remove an over-the-scope-clip (with video). Gastrointest Endosc 2013;77:974–975. [ Links ]
Statement of Ethics
This study did not require informed consent or review/approval by the appropriate ethics committee.
Disclosure Statement
The authors have no conflicts of interest to declare.
* Corresponding author.
Dr. Marta Rocha
Department of Gastroenterology
Hospital de Santo António, Centro Hospitalar do Porto Largo Prof. Abel Salazar
PT–4099-001 Porto (Portugal)
E-Mail martalemosrocha@gmail.com
Received: November 25, 2017; Accepted after revision: January 18, 2018

