










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.27 no.1 Lisboa fev. 2020
https://doi.org/10.1159/000500144
CLINICAL CASE STUDY
Hepatic Adenomatosis: A Challenging Liver Disease
Adenomatose hepática: uma doença hepática desafiante
Diana Leite Gonçalvesa, José Pedro Leitea, Rafael Silvaa, António Pedro Pissarrab, Rui Caetano Oliveirac,Dilva Silvaa
aDepartment of Internal Medicine, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal; bDepartment of Radiology, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal; cDepartment of Anatomical Pathology, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal
* Corresponding author.
ABSTRACT
Hepatic adenomatosis is defined as the presence of 10 or more adenomas in an otherwise normal liver. Half of the cases are clinically silent and detected incidentally in imaging exams. A 42-year-old woman with previous history of arterial hypertension and mixed dyslipidemia had multiple liver nodules incidentally identified in an abdominal computed tomography scan. She was asymptomatic and her physical examination was unremarkable but laboratory analysis revealed increased alkaline phosphatase and mildly persistent elevated systemic inflammatory markers. A subsequent hepatic magnetic resonance imaging (MRI) suggested the diagnosis of hepatic adenomatosis and the liver biopsy confirmed the presence of inflammatory adenomas. The patient stopped oral contraception and, at 6 months of follow-up, laboratory inflammatory markers had normalized. She is now under biannual follow-up with MRI and alpha-fetoprotein dosing. This case provides an example of the complex management of this disease in terms of diagnosis, treatment, and follow-up.
Keywords: Adenoma, Inflammation, Oral contraception, Treatment, Follow-up
RESUMO
A adenomatose hepática define-se pela presença de 10 ou mais adenomas num fígado normal. Cerca de metade dos casos são silenciosos e de identificação incidental em exames de imagem. Uma mulher de 42 anos, com antecedentes pessoais de hipertensão arterial e dislipidémia mista, realizou uma tomografia computorizada abdominal, com identificação incidental de múltiplos nódulos hepáticos. Apresentava-se assintomática e sem alterações ao exame objetivo mas as análises laboratoriais revelaram fosfatase alcalina elevada e aumento ligeiro mas persistente dos parâmetros inflamatórios sistémicos. A ressonância magnética hepática (RMH) subsequente sugeriu o diagnóstico de adenomatose hepática e a biópsia de nódulo confirmou a presença de adenoma do tipo inflamatório. Foi suspensa a toma de contraceptivo oral e, aos 6 meses de follow-up, observou-se normalização dos parâmetros inflamatórios. Actualmente encontra-se sob vigilância semestral com RMH e doseamento de alfa-fetoproteína. Este caso representa a complexidade inerente à abordagem do diagnóstico, tratamento e follow-up da adenomatose hepática.
Palavras-chave: Adenoma, Inflamação, Contracepção oral, Tratamento, Seguimento
Introduction
Hepatocellular adenomas (HCA) are an uncommon benign neoplasm, first described in 1861 by Frerichs [1], which became widely recognized in the 1960s and 1970s following the introduction of oral contraceptive pills (OCP) [2]. HCA have a global reported incidence of 3/1,000,000/year, but this number is substantially higher in women with long-term OCP use, estimated to be 3–4/100,000/year [1]. Hepatic adenomas are mostly single, usually located in the right lobe, but several simultaneous lesions in liver parenchyma may be seen. In 1985, Flejou et al. [3] described hepatic adenomatosis, referring to cases where more than 10 adenomas were present in an otherwise normal liver. HA has an incidence of 10–24% in patients with hepatic adenoma [1]. Approximately half the cases are clinically silent and detected incidentally, making the diagnosis of HCA and HA a challenging process that requires a strong clinical suspicion, combination of imaging studies, and histological confirmation [4]. The complications associated with HA, like malignant transformation, rupture, and bleeding, can be life threatening. This case report aims to highlight the importance of prompt recognition of HCA and HA and the need for better understanding of this disease in order to optimize its management.
Case Presentation
We describe the case of a 42-year-old white woman referred to an internal medicine appointment by her primary care physician in order to exclude a secondary cause of hypertension. The patient had been diagnosed with hypertension and mixed dyslipidemia 10 years before and was medicated with losartan 50 mg i.d., hydrochlorothiazide 12.5 mg i.d., and atorvastatin 20 mg i.d., with a normal lipid profile but poorly controlled hypertension. She had a smoking history of 13 pack years and was under combined OCP for the last 17 years. Apart from this, there was no other relevant personal or family history. She denied taking any over-the-counter medication and the use of recreational drugs. She was asymptomatic and her physical examination, including blood pressure and temperature, was unremarkable. Her body mass index was 21.22.
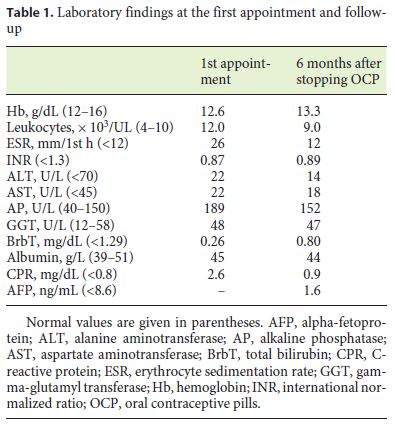
Initial laboratory investigation (Table 1) revealed an elevated serum alkaline phosphatase (AP; 189 U/L, normal < 126 U/L), Creactive protein (CRP; 2.6 mg/dL, normal < 0.5 mg/dL) and erythrocyte sedimentation rate (ESR; 26 mm/h, normal < 12). Her blood count, coagulation tests, renal function, sodium, and potassium were normal, as were the levels of bilirubin, transaminases, and albumin.
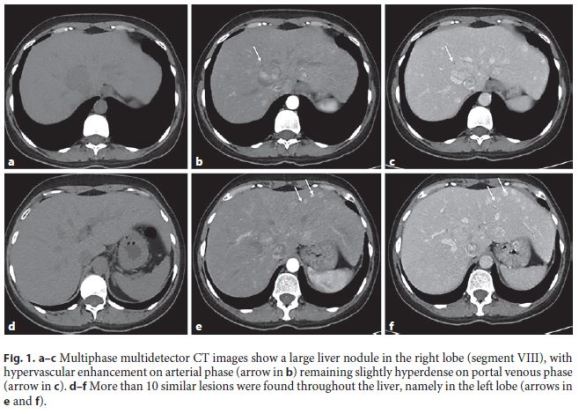
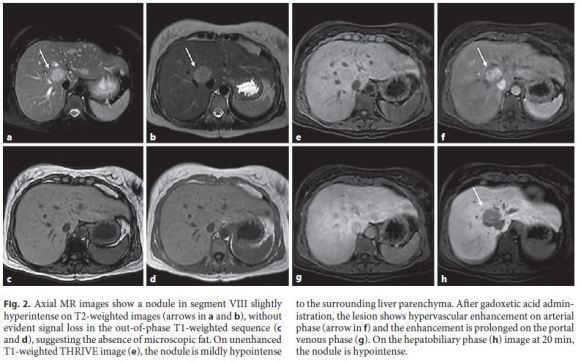
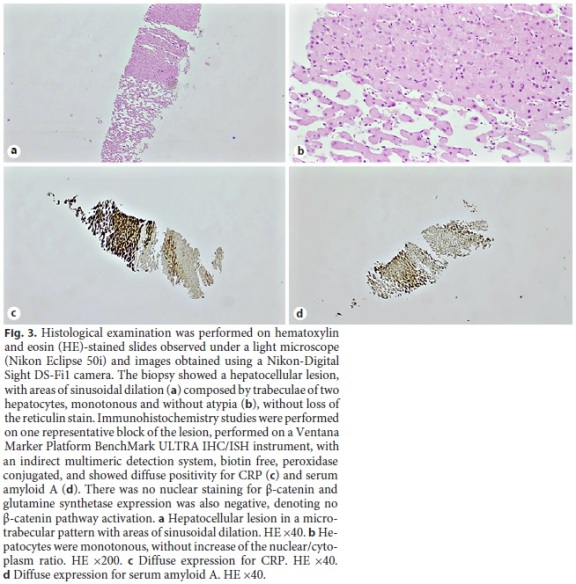
An abdominal computed tomography (CT) scan was performed, intending to rule out the presence of an adrenal adenoma/hyperplasia as the cause of hypertension, and identified more than 10 hepatic nodules (Fig. 1), the largest in the 8th segment with a greater axis of 3.7 cm. There were no other relevant changes. A subsequent hepatic magnetic resonance image (MRI) was performed (Fig. 2) showing that the liver lesions were slightly hyperintense on T2-weighted images, with hypervascular enhancement on the arterial phase, remaining hyperintense on the portal venous phase and hypointense on the hepatobiliary phase, findings suggesting the diagnosis of HA. Due to the permanently elevated CPR and ESR, associated with multiple liver nodules of unknown cause, investigation was extended with a serum protein electrophoresis, alpha-fetoprotein, an upper gastrointestinal endoscopy, and a colonoscopy, all of which were normal or unremarkable. The patient underwent CT-guided hepatic biopsy (Fig. 3) that confirmed the diagnosis of HA (inflammatory type, without β-catenin mutation).
The case was presented and discussed in a multidisciplinary team and since the risk of complications, namely adenoma rupture, bleeding, or malignant transformation, was considered low, a conservative attitude was adopted, with biannual imaging and laboratory follow-up. She stopped OCP and, as a contraception method, was submitted to tubal ligation. Six months after the diagnosis and OCP cessation, the number and size of nodules remained identical, but laboratory inflammatory markers and AP progressively declined to normal values (Table 1). One year after diagnosis the patient is well and asymptomatic, with good control of arterial hypertension and dyslipidemia under perindopril 10 mg, bisoprolol 5 mg, amlodipine 5 mg, and atorvastatin 20 mg once daily.
Discussion
HCA and HA were traditionally considered distinct entities but nowadays they are thought to share the spectrum of the same disease process [4, 5]. Their characteristics in terms of gender, risk factors classification, and treatment and surveillance are summarized in Table 2.
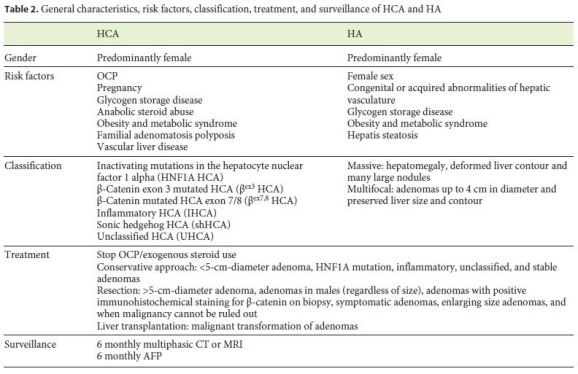
In 2006 a French collaborative group (Bioulac-Sage et al. [6]) introduced a phenotype-genotype classification to categorize adenomas [5, 6]. Recently, major advances have improved the knowledge of the molecular mechanisms underlying HCA development [7]. Nowadays HCA can be classified into 6 major subgroups (Table 2) [7]. As described for our patient, HA is generally asymptomatic, although symptoms may be present, most often mild, such as right upper quadrant discomfort or bloating [5].
Chiche et al. [8] suggested two forms of HA: massive and multifocal (Table 2). Patients with the latter form are unlikely to have symptoms and appear to have a less aggressive clinical course, as it was observed in our case. Liver laboratory analysis may be abnormal (elevated serum AP and gamma-glutamyl transferase) when a space-occupying tumor is present but especially when there is necrosis or hemorrhage associated [1, 9]. In our case, the largest adenoma had a greater axis of only 3.7 cm without evidence of necrosis or hemorrhage. The laboratory changes may be explained by the high number of lesions observed.
Inflammatory adenomas account for 35–45% of HCA cases and generally occur in obese patients and those with metabolic syndrome or systemic inflammatory syndromes [1, 2, 4]. They are characterized by intralesional inflammatory infiltration and increased serum amyloid-A and CRP expression. Inflammatory anemia or fever can sometimes be observed in these patients and possibly be considered paraneoplastic syndromes induced by the uncontrolled production of cytokines [7]. Sinclair et al. [10] described the case of a woman with important systemic inflammatory symptoms and biochemical signs of inflammation related to hepatic inflammatory adenomas which resolved after OCP cessation. In our case the persistent elevation of CRP and ESR alerted us to the possibility of a systemic disease or occult malignancy even though the patient was asymptomatic. The additional investigation performed minimized this concern while hepatic biopsy, the gold standard method for diagnosis [1], confirmed the presence of HA due to inflammatory adenomas. Even though there is no established relation between HA and OCP (Table 2), in this case, normalization of liver laboratory analysis and systemic inflammatory markers was observed after OCP cessation, despite the tumors being the same number and size on follow-up. On the other hand, isolated hepatic adenomas clearly show regression with cessation of exogenous steroid use [1, 5].
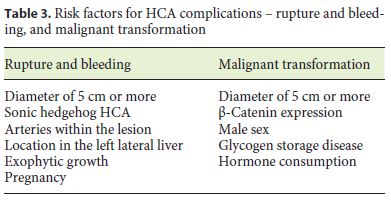
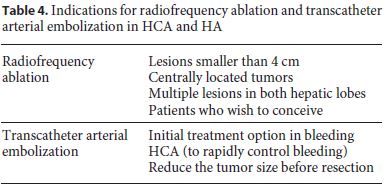
The natural history and prognosis of HA are still not very clear and there lacks consensus regarding the management for this disease. Classically, HCA treatment was surgical resection because it was believed to have potential for malignant transformation and/or bleeding. However, the better knowledge of HCA, and consequently HA, has changed the paradigm of its management. Today, it is not only the established risk of complications (Table 3), but also the molecular subtyping of the adenoma that defines the indication for surgical resection of lesions (Table 2). Malignant transformation is rare but known to occur in any subtype, though it is more often in βex3 HA [1, 5, 7]. Inflammatory adenomas have a 30% incidence of hemorrhage and a 5–10% incidence of β-catenin mutations [5]. βex3 adenomas in HA may require an oncologic resection as it may be difficult to differentiate from hepatocellular carcinoma on biopsy [8]. Sometimes surgical resection can be impractical and liver transplantation may be necessary, being the last therapeutic option [11]. On the other hand, radiofrequency ablation and transcatheter arterial embolization are less invasive treatment options with specific indications (Table 4) [1].
Although it was not a concern factor in this case, special considerations should be taken in pregnant women with HA, since the risk of the hormone-induced growth and spontaneous rupture of a tumor can threaten the life of the mother and child. Pregnancy is not contraindicated, but if HCA larger than 5 cm are present, they should be resected before conception [1].
There are no clear recommendations for surveillance, but a biannual control with CT or MRI and alpha-fetoprotein is generally accepted [1, 4]. Our patient did not have any risk factors for complications, so we opted for biannual follow-up. A year after diagnosis and suspension of OCP, she is asymptomatic with normalization of inflammatory markers, without any evidence of disease evolution.
Conclusion
HA is a rare disease that provides a clinical challenge since it is not fully understood in its physiopathology, approach, and management. Its definite diagnosis requires an excisional biopsy in the majority of situations. The prevention of its complications is extremely important and treatment, which has recently evolved through the development of molecular subtypes, should be adapted to each case.
References
1 Begum S, Khan MR. Hepatocellular adenoma: review of contemporary diagnostic and therapeutic options. IJS Short Rep. 2018;3(1):1–8. [ Links ]
2 Chang CY, Hernandez-Prera JC, Roayaie S, Schwartz M, Thung SN. Changing epidemiology of hepatocellular adenoma in the United States: review of the literature. Int J Hepatol. 2013; 013:604860.
3 Flejou JF, Barge J, Menu Y, Degott C, Bismuth H, Potet F, et al. Liver adenomatosis. An entity distinct from liver adenoma? Gastroenterology. 1985 Nov;89(5):1132–8. [ Links ]
4 Yang MJ, Hernandez-Gonzalo D, Thomas EM. A case of extensive hepatic adenomatosis in a renal transplant patient. J Surg Case Rep. 2018 Aug; 2018(8):rjy195. [ Links ]
5 Low G, Dharmana H, Saravana-Bawan S, Girgis S. Case 235: Hepatic Adenomatosis Due to Inflammatory Adenomas. Radiology. 2016 Nov;281(2):639–45. [ Links ]
6 Bioulac-Sage P, Cubel G, Taouji S, Scoazec JY, Leteurtre E, Paradis V, et al. Immunohistochemical markers on needle biopsies are helpful for the diagnosis of focal nodular hyperplasia and hepatocellular adenoma subtypes. Am J Surg Pathol. 2012 Nov;36(11):1691–9. [ Links ]
7 Nault JC, Paradis V, Cherqui D, Vilgrain V, Zucman-Rossi J. Molecular classification of hepatocellular adenoma in clinical practice. J Hepatol. 2017 Nov;67(5):1074–83. [ Links ]
8 Chiche L, Dao T, Salame E, Galais MP, Bouvard N, Schmutz G, et al. Liver adenomatosis: reappraisal, diagnosis, and surgical management: eight new cases and review of the literature. Ann Surg. 2000 Jan;231(1):74–81. [ Links ]
9 Donato M, Hamidian Jahromi A, Andrade AI, Kim R, Chaudhery SI, Sangster G. Hepatic adenomatosis: a rare but important liver disease with severe clinical implications. Int Surg. 2015 May;100(5):903–7. [ Links ]
10 Sinclair M, Schelleman A, Sandhu D, Angus PW. Regression of hepatocellular adenomas and systemic inflammatory syndrome after cessation of estrogen therapy. Hepatology. 2017 Sep;66(3):989–91. [ Links ]
11 Fernandez-Vega I, Santos-Juanes J, Garcia-Pravia C, Fresno-Forcelledo MF, Rodrigo L. Hepatic adenomatosis: a rare cause of liver transplant. Rev Esp Enferm Dig. 2014 Aug;106(7):494–6. [ Links ]
Statement of Ethics
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Sources
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
* Corresponding author.
Diana Leite Goncalves
Department of Internal Medicine, Centro Hospitalar e Universitario de Coimbra
Rua Principal, No. 455, Logo de Deus
PT–3020-212 Coimbra (Portugal)
E-Mail dianafslg@gmail.com
Received: January 22, 2019; Accepted after revision: March 29, 2019
Author Contributions
D.L.G. conceived of the manuscript, which was drafted together with J.P.L. and R.S. A.P.P., R.C.O., and D.S. participated in the review process and coordination. All the authors critically revised the manuscript and provided final approval of the version to be submitted.

