










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.27 no.1 Lisboa fev. 2020
https://doi.org/10.1159/000500609
IMAGES IN GASTROENTEROLOGY AND HEPATOLOGY
Polypoid Gastric Heterotopia of Colon
Heterotopia gástrica polipóide do colon
Marcela Adriana Duran Alvareza, Carla Noemi Tafur Sanchezb
aDepartment of Pathology, Hospital de Medina del Campo, Valladolid, Spain; bDepartment of Gastroenterology, Hospital de Medina del Campo, Valladolid, Spain
* Corresponding author.
Keywords: Gastric heterotopia, Gastric mucosa, Colonic polyps
Palavras-chave: Heterotopia gástrica, Mucosa gástrica, Pólipos colónicos
Clinical Case
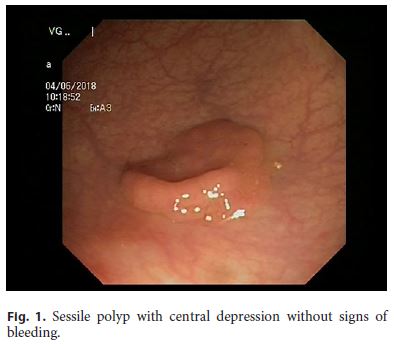
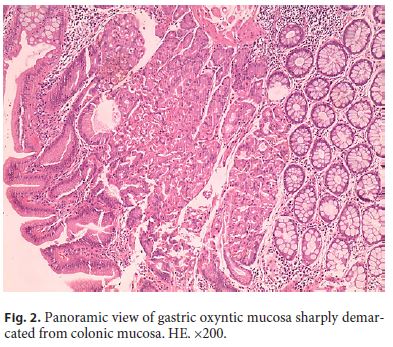
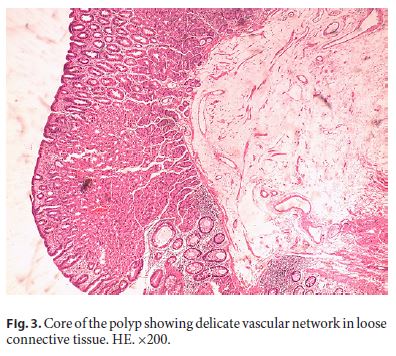
A 67-year-old male presented to the Emergency Department with watery diarrhea of 2 days’ duration with intermittent rectal bleeding without fever, vomiting, or abdominal pain. His clinical history included the diagnosis of irritable bowel 10 years ago, hypertension, ischemic cardiopathy, dyslipidemia, abdominal aneurysm, and hiatal hernia. He was in treatment with furosemide, fenofibrate, salicylate, and omeprazole. Physical examination was unremarkable except for the presence of hemorrhoids, although rectal touch was negative. Blood test excluded anemia or signs of an infectious disease. For the first time, the patient underwent a colonoscopy that identified two polyps. One was a tubular adenoma with low-grade dysplasia, without signs of bleeding, measuring 3 mm in diameter, located at 40 cm from the anal verge. The second was a sessile nonulcerated polyp, centrally depressed (Fig. 1), measuring 20 mm, located at 20 cm from the anal verge. Histologically, this polyp was entirely covered by an intact gastric oxyntic mucosa with all the elements found in normal orthotopic oxyntic mucosa (Fig. 2), sharply demarcated from the surrounding colonic mucosa (Fig. 3). The core of the polyp showed loose connective tissue with a fine vascular network without signs of bleeding or thrombosis. Neither epithelial dysplasia nor malignancy were detected. The diagnosis was polypoid gastric heterotopia of the colon (GH).
Discussion
The presence of heterotopic gastric mucosa in the colon is a rare finding of unclear pathogenesis probably related to a developmental error in gastric positioning and migration along the early embryonic life [1]. Microscopically, almost all reported cases are of oxyntic type [1–4]. All the normal components of oxyntic mucosa are present and functioning [1–4]. In contrast, gastric metaplasia is usually of pyloric type and arises in a chronic inflammatory background by reprogramming differentiation of reserve cells in the colonic crypts; therefore, the structure of normal gastric mucosa is not present [1, 2].
This entity has been described in children and adults. Episodic diarrhea, rectal bleeding and abdominal pain are common symptoms. Often, the patients were diagnosed as having irritable bowel [1, 2]. GH can be multifocal and accompanied by other intestinal and extraintestinal malformations [1, 2]. The diagnosis of colonic GH should prompt the search for other intestinal lesions by abdominal computed tomography, capsule endoscopy, and/or technetium-99m pertechnetate scan. In some cases, the source of bleeding was identified in the surrounding colonic mucosa as a corrosive effect of acid secretion [2]. In our case, no other lesions were detected on colonoscopy, and we considered that hemorrhoids could be the source of bleeding. Our patient was in treatment with omeprazole because of his hiatal hernia. We suspect that a fault in the omeprazole treatment could precipitate this episode.
Treatment of polypoid GH is endoscopic resection. In one reported case, treatment with a H2-antagonist was used with success in the control of bleeding [3]. Colonic adenocarcinoma in GH has been described in the literature [4], but the link between these two entities is unclear. No other lesions were found in the workup. Omeprazole was not maintained. Twelve months after polypectomy, the patient is doing well.
References
1 Srinivasan R, Loewenstine H, Mayle JE. Sessile polypoid gastric heterotopia of rectum: a report of 2 cases and review of the literature. Arch Pathol Lab Med. 1999 Mar;123(3):222–4. [ Links ]
2 Fenoglio-Preiser CM. Gastrointestinal Pathology. Wolters Kluwer ed. Philadelphia; 2008. pg. 857–8. [ Links ]
3 Murray FE, Lombard M, Dervan P, Fitzgerald RJ, Crowe J. Bleeding from multifocal heterotopic gastric mucosa in the colon controlled by an H2 antagonist. Gut. 1988 Jun;29(6):848–51. [ Links ]
4 Ko H, Park SY, Cha EJ, Sohn JS. Colonic adenocarcinoma arising from gastric heterotopia: a case study. Korean J Pathol. 2013 Jun;47(3):289–92. [ Links ]
Statement of Ethics
This study did not require informed consent or review/approval by the ethics committee.
Disclosure Statement
All authors have read and approved the manuscript and declare that they have no conflict of interests.
* Corresponding author.
Marcela Adriana Duran Alvarez
Department of Pathology, Hospital de Medina del Campo
Carretera de Peñaranda, s/n
ES–47400 Valladolid (Spain)
E-Mail marduran12@yahoo.es
Received: April 5, 2019; Accepted after revision: April 12, 2019
Acknowledgements
The authors want to thank Mr. Jose Eduardo Matos (photographer) for his technical assistance.
Author Contributions
M.A.D.A.: design, search, drafting the manuscript including histologic images. C.N.T.S.: management of the patient, search, and endoscopic image.

