











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkMost cases of acute, sharp, flank pain radiating to the scrotum or groin are caused by nephrolithiasis or ureterolithiasis and are commonly referred to as renal colic. Computed tomography (CT) has become a standard imaging technique for uncomplicated renal colic in many countries [1], revealing an alternative diagnosis in up to 6% of the patients [1].
Although rare, gastrointestinal perforation by a foreign body may be associated with hydronephrosis, due to the contiguous inflammatory process, and present itself as flank pain [2]. Fishbone ingestion with bowel perforation is a particularly challenging diagnosis as the presentation may mimic common abdominal pathologies, and patients may not recall the ingestion of a foreign body [3].
The following case highlights the diagnostic difficulties in considering and identifying alternative etiologies for flank pain and its possible association with gastrointestinal perforation by a foreign body.
The authors present a case of a 63-year-old woman admitted to the emergency room department with a constant, sharp, right flank pain lasting for a week. No urinary, gastrointestinal, or constitutional symptoms were present. On physical examination, the right renal murphy sign was present with no other abnormal findings.
The only laboratory finding was an elevated C-reactive protein (76.58 mg/L). Renal ultrasound demonstrated renal pelvis dilation but showed no nephrolithiasis or other causes of obstruction. A CT scan without contrast revealed a foreign body intersecting the third portion of the duodenum, the ureter, and the psoas muscle, associated with dilation of the proximal ureter and renal pelvis and densification of the surrounding fat (Fig. 1a, b).
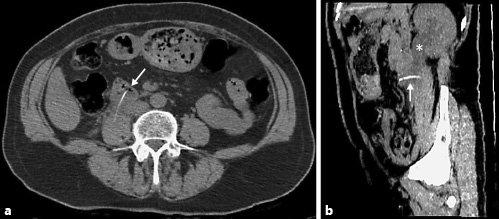
Fig. 1 CT scan showing a foreign body perforating the third portion of the duodenum and crossing the ureter and the psoas muscle (arrow), resulting in hydronephrosis (asterisk). a Axial reconstruction; b sagittal reconstruction.
An esophagogastroduodenoscopy was performed for diagnostic and therapeutic purposes. During the procedure, a fishbone embedded in the wall of the third portion of the duodenum was identified and removed with a foreign body forceps (Fig. 2a, b).
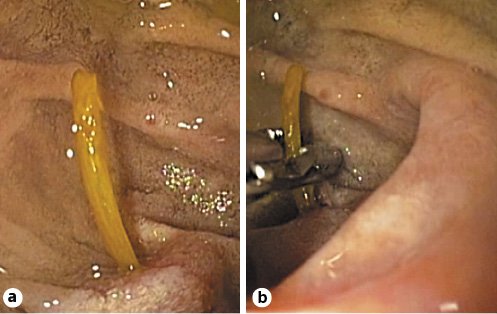
Fig. 2 Esophagogastroduodenoscopy images showing a foreign body (fishbone) embedded in the duodenum wall (a) and its’ removal with a foreign body forceps (b).
Following the procedure, the patient started intravenous antibiotics and fluids. Oral feeding was reintroduced after 2 days. She was discharged completely asymptomatic after 7 days.
At the 3-month follow-up, the review CT scan with contrast showed complete resolution of the previously observed pathological findings and normal excretion of contrast by the right kidney (Fig. 3a, b).
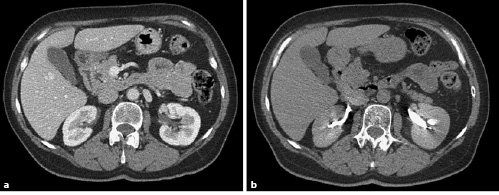
Fig. 3 CT scan (axial reconstruction) showing normal contrast uptake (a) and excretion (b) by the right kidney.
Gastrointestinal perforation by a foreign body may present itself in various forms, some of which may be difficult to diagnose. CT continues to be the gold standard for diagnosis of the etiology of renal colic.

