











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
A Caucasian 60-year-old man, with a career in house-building, presented with mild, chronic and progressive dysphagia, manifested by difficulty in swallowing solid food for the last 6 months. He had no cervical pain, weight loss, dysphonia, respiratory complaints, previous surgical intervention, radiotherapy, major trauma, myogenic or metabolic known causes for this symptom. The patient had a normal cervical and chest physical examination and neurologic exam. A barium swallow test was firstly performed, revealing a posterior esophagus indentation due to an osteophyte formation, which interfered with contrast progression. This exam also ruled out dysfunction in motility or a Zenker’s diverticulum. Consequently, to better characterize the osteoarticular disease, the patient was submitted to a computed tomography (CT) and cervical magnetic resonance imaging (MRI) which revealed degenerative changes such as: anterior and lateral protrusion of vertebral discus, osteophytes from C3 to C5, uncarthrosis, and posterior C3 to C6 interapophysary hypertrophic arthrosis, without ligament calcification or cervical webs (Fig. 1a-c). Finally, upper digestive endoscopy ruled out intrinsic abnormalities, and cervical ultrasound was also normal.
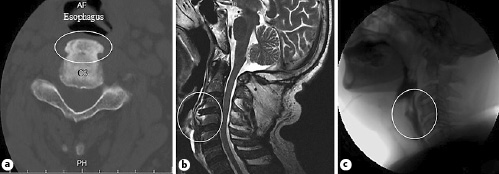
Fig. 1 a C3 somatic marginal osteophyte (white circle) on CT. b Cervical MRI with anterior and lateral protrusion of the vertebral discus and osteophytes in C3 to C5. c Barium swallows with posterior esophagus indentation at the level of the osteophyte formation.
Cervical osteophytes occur in 20-30% of the general population [1] and are mostly associated with diffuse idiopathic skeletal hyperostosis and ankylosing spondylitis [2]. Most osteophytes of the anterior margin of the cervical spine are asymptomatic. Nevertheless, cervical osteophytes were the cause of dysphagia in 11.7% of a studied population, with a mean age of 79 ± 8 years [3, 4], disclosing a possible underrecognized etiology. In this matter, according to Lee et al. [5], patients with this condition were usually men (81%), with a mean age of 68 years and the C3 to C6 level most commonly involved, typically presenting with a long history of dysphagia. Other symptoms include food impaction, dysphonia and respiratory obstruction [2, 3]. The diagnostic imaging approach includes a lateral X-ray, barium swallow, and cervical CT or MRI. Surgical approach may be a definite solution, but diet restrictions may cause satisfactory improvement [1-3, 5]. Our patient was paucisymptomatic and remains only with adapted diet. The authors highlight anterior cervical osteophytosis as a differential diagnosis of oropharyngeal dysphagia.

