











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
sions with submucosal endoscopic appearance [2]. Metastases in the gastric mucosa are even rarer, with a reported incidence of 0.2-0.7% among patients with non-hematologic malignancies in postmortem studies [3].
Testicular germ cell tumors metastasize to the gastrointestinal tract in about 5% of cases, most of these evolving in the small intestine and manifesting as bowel obstruction or, less frequently, as gastrointestinal bleeding [4]. They are classified as seminomas and nonseminomas. Seminomas are the least likely testicular tumor to metastasize to the gastrointestinal tract, with an incidence of 1% in a 486-post-mortem-cases study [4]. We report a rare case of a previously undiagnosed testicular seminoma presenting as upper gastrointestinal bleeding due to multiple metastases to the gastric mucosa.
Case Report
A 45-year-old man without past medical history was admitted to the emergency room with weight loss (11% of total body weight in 2 months), asthenia, and fever, followed by melaena. The initial work up revealed a severe normocytic normochromic anemia (hemoglobin at 4.1 g/dL, normal range [NR]: 13.0-17.7) and markedly elevated lactate dehydrogenase (2,231 U/L, NR: 100-247). Upper endoscopy showed three atypical-looking ulcers in the greater curvature of the gastric body, one of which with a visible vessel successfully submitted to endoscopic hemostasis with two through-the-scope clips after diluted adrenalin injection (1:10,000) in and around the ulcer base (shown in Fig. 1). Biopsies of the ulcers were performed. Abdominal computed tomography revealed an extensive heterogeneous retroperitoneal mass with a diameter of 15 cm, causing inferior vena cava stenosis, and a right pelvic mass with a diameter of 10 cm (shown in Fig. 2). The laboratory evaluation was notable for neuron-specific enolase of 168.5 ng/mL (NR: < 12.5). Prostate-specific antigen, carcinoembryonic antigen, alpha-feto-protein, cancer antigens 19-9 and 72-4, immunoglobulin levels, protein electrophoresis, immunophenotyping of peripheral blood and human immunodeficiency virus serology were negative. Gastric ulcers’ biopsies revealed a highly proliferative neoplasia of unknown origin, dissociated from the gastric glandular component, with immunohistochemical positivity for cluster of differentiation (CD) 56, CD117, CD68, CD10, and CD99 and negativity for cytokeratins, CD3, CD5, CD20, CD23, B-cell lymphoma 2, B-cell lymphoma 6, cyclin D1, melan-A, myeloperoxidase, and neuroendocrine markers (shown in Fig.3a-d). The retroperitoneal mass biopsy showed an undifferentiated neoplastic proliferation with similar histologic findings and immunohistochemical profile (shown in Fig. 3e). The remaining study performed over the following weeks was unremarkable, including head, neck, chest, and lumbar/dorsal spine computed tomography; prostatic ultrasound; and colonoscopy. One month after the initial presentation, upper endoscopy was repeated under deep sedation. Similar findings were observed (shown in Fig. 1), and multiple biopsies of the ulcers were taken. At this point, the patient complained of an enlarged right hemiscrotum suggestive of a testicular tumor in testicular ultrasound. A radical orchiectomy was performed. Histopathologic findings were compatible with a pure testicular seminoma (shown in Fig. 3f), with tunica albuginea and spermatic cord invasion. Revision of both gastric and retroperitoneal biopsies was compatible with metastatic seminoma. Further laboratory study revealed an elevated β-human chorionic gonadotropin (29.4 IU/L, NR: < 0.5) and persistently normal alphafetoprotein. With an IIIC stage (T3N3M1bS2) [5], the patient underwent chemotherapy with bleomycin, etoposide, and platinum. Because of an incomplete response of the retroperitoneal mass, not resectable due to vascular adherences, the patient is undergoing radiotherapy. There was no hemorrhagic recurrence.
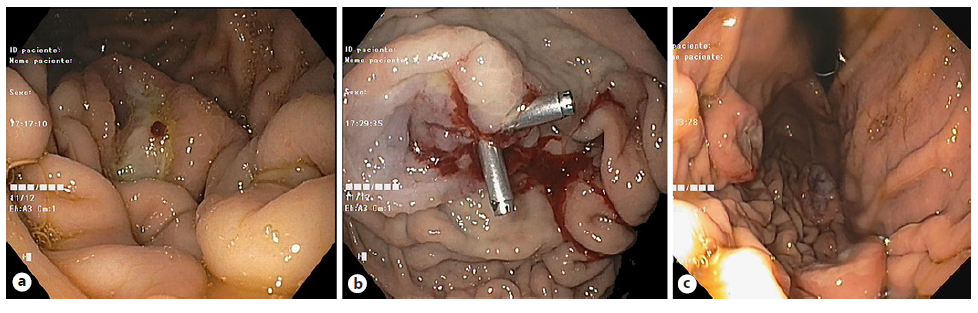
Fig. 1 Atypical “volcano-like” gastric ulcers. a, b One of the ulcers with a visible vessel that was submitted to endoscopic hemostasis. c Four-week re-evaluation with repeated biopsies.
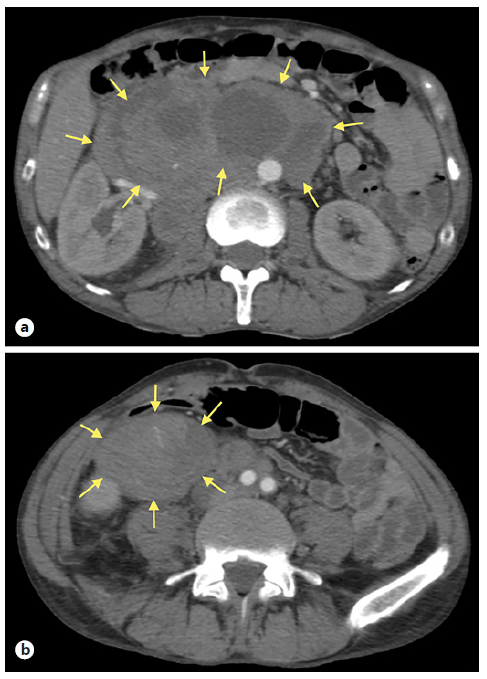
Fig. 2 Abdominal computed tomography findings. a An extensive heterogeneous retroperitoneal mass with a diameter of 15 cm. b A right pelvic mass with a diameter of 10 cm.
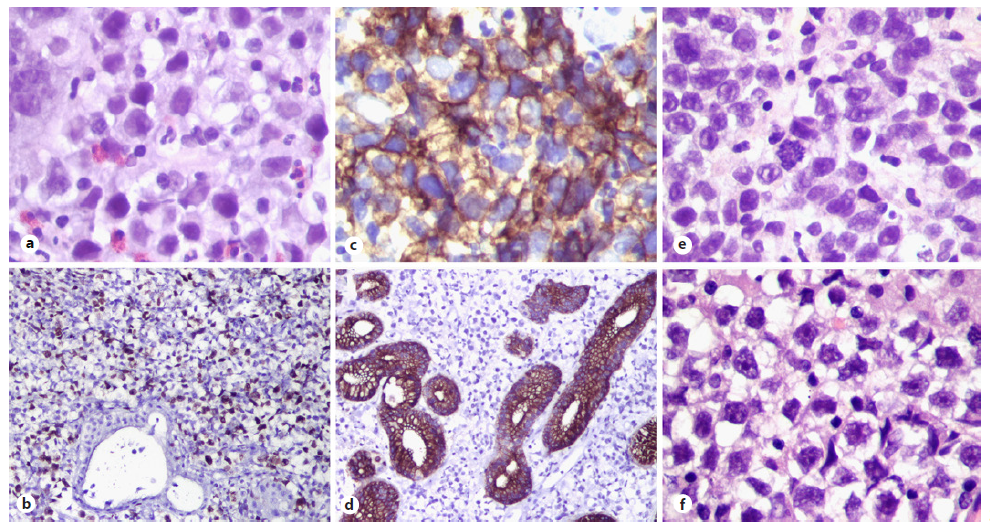
Fig. 3 Histologic findings: gastric biopsies revealing large cells with big hyperchromatic nuclei and prominent nucleoli, independent from the gastric glandular component (a, hematoxylin and eosin, ×400), with high proliferation index (Ki-67, b, ×100), positivity for CD117 (c, ×400), and negativity for cytokeratins (d, ×100). Identical findings in the retroperitoneal mass biopsy (e, ×400) and in the testicular tumor specimen (f, ×400).
Discussion/Conclusion
Metastatic involvement of the stomach arising from testicular germ cell tumors is rare and usually detected after the primary tumor is diagnosed [1]. We report a case in which the first presentation was gastrointestinal bleeding arising from gastric metastases. The multiplicity of gastric lesions with mucosal involvement, suggesting a hematogenous route, is an even rarer finding [3].
Contrary to our case, most germ cell tumors with gastric metastasis have a nonseminoma component [6]. There are few reported cases of pure seminoma presenting at diagnosis with gastric metastases, both with and without macroscopic retroperitoneal ganglia involvement [7-9]. Most of these cases report a single gastric metastasis and some are associated with other visceral organ metastases, unlike our patient.
This case highlights the importance of the differential diagnosis of malignant gastric ulcers. The hypothesis of a germ cell tumor should be considered in cases where biopsies reveal a poorly differentiated neoplasm, particularly in young men with severe anemia. In our particular case, since a retroperitoneal mass was diagnosed at admission, a germ cell tumor should have been considered earlier in the diagnostic work up. The marked elevation of lactate dehydrogenase was in accordance with this hypothesis. Direct questioning about scrotal swelling, genital examination, dosing of the tumor marker β-human chorionic gonadotropin, and a low threshold for the performance of a testicular ultrasound would have been crucial for a prompter diagnosis. In addition, an early second opinion from a more specialized pathologist would have been appropriate.
A prompt diagnosis is of particular importance in the setting of a testicular seminoma, in which the presence of metastatic disease does not preclude a curative approach. In fact, all seminomas are categorized as having good or intermediate prognosis. In our case, the presence of nonpulmonary visceral metastases warrants an intermediate prognosis, with 88% 5-year survival rate [10]. However, lactate dehydrogenase elevation was recently redefined as an independent adverse prognostic marker [10], and there are insufficient data to predict the outcome in the infrequent scenario of gastric involvement by metastatic disease.
In conclusion, we report a rare initial presentation of testicular seminoma as gastrointestinal bleeding due to gastric metastases, emphasizing one of the unusual man-ifestations of germ cell malignancies and highlighting the importance of detailed anamnesis and physical examination in the differential diagnosis of atypical gastric ulcers.

