











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkA 70-year-old male patient underwent his first upper endoscopy for anemia work-up. Beyond a 3-cm hiatal hernia, an endoscopic diagnosis of Barrett’s esophagus (Prague classification C3M4) was entertained, as illustrated by a tongue at 3 o’clock on blue laser imaging (Fig. 1a). However, at the gastroesophageal junction an estimated 20-mm nodular, superficially ulcerated lesion emerged (Fig. 1b), likewise visualized on linked color imaging (LCI) after intra-hernial retroflexion (Fig. 1c). Giv en this presumed malignant complication, full-scale assessment of the Barrett’s esophagus was warranted, including acetic acid spraying. In combination with LCI, another 8-mm utterly flat lesion emerged at 6 o’clock with an irregular vessel and surface pattern, highly suggestive of early cancer as a second lesion (Fig. 1d). Pathology of endoscopic biopsies confirmed specialized intestinal metaplasia and, more intriguingly, indicated a well-differentiated adenocarcinoma (AC) for the flat lesion (Fig. 2a) and a poorly differentiated squamous cell carcinoma (SCC) for the nodular lesion (Fig. 2b). Cross-sectional and EUS staging indicated T1/2N+ stage. Notwith-standing, due to advanced chronic obstructive pulmonary disease (GOLD IIIB with long-term oxygen therapy), the patient underwent upfront esophagectomy without significant complications after pulmonary prehabilitation. Final surgical pathology indicated pT1a, pN0(0/27), G1 for the AC and pT1b, pN1(2/27), G3 for the SCC (furthermore: L0, V0, Pn0, R0 each).
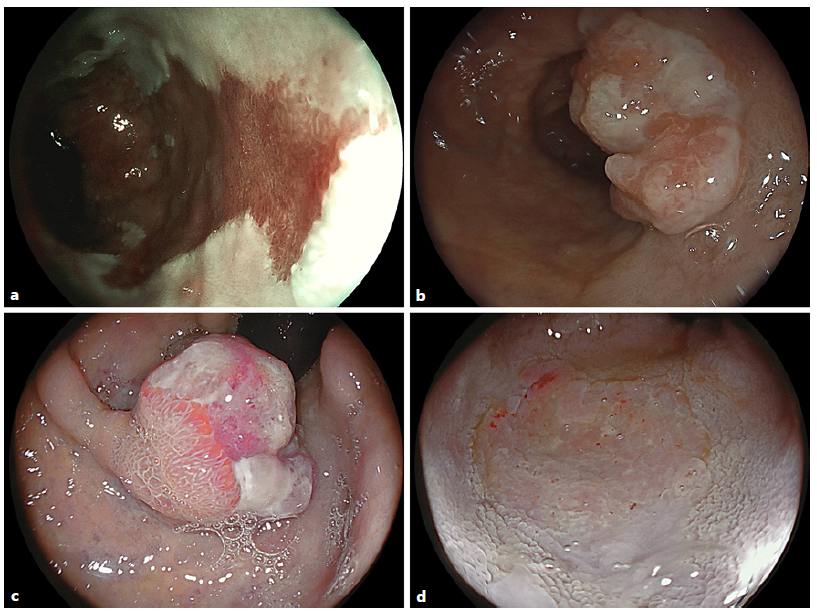
Fig. 1 a Blue laser imaging of a Prague C3M4 Barrett’s esophagus with a tongue highlighted at 3 o’clock. b An estimated 20-mm nodular ulcerated lesion emerged at the gastroesophageal junction (c) as replicated on retroflexed LCI visualization. d LCI after acetic acid spraying in the distal esophagus highlighted another 8-mm flat lesion with an irregular vessel and surface pattern consistent with early cancer.
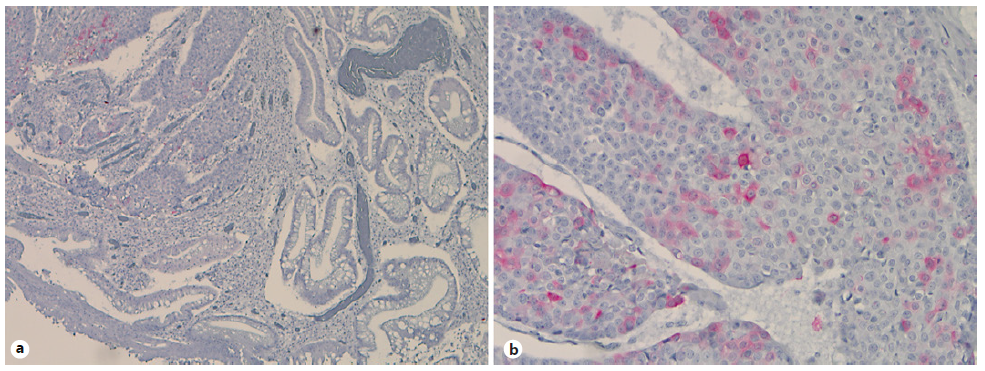
Fig. 2 Immunohistochemistries for cytokeratin (CK) 5/6 with negative staining of the AC (a) and positive results in the SCC (b).
Barrett´s esophagus is a well-acknowledged risk factor for esophageal AC formation; however, singular cases of SCC arising in Barrett’s esophagus and/or collision tumor comprising SCC and AC elements have been documented in the literature, pointing to ambivalent carcinogenic field effects [1-3]. Concurrent SCC and Barrett’s carcinoma has occasionally been reported in Barrett’s esophagus before, however, to the best of our knowledge, not with the Barrett’s segment itself [4-6]. Of interest, the patient had a mixed risk profile, including obesity and metabolic syndrome (Barrett’s) and heavy smoking (SCC). The distinct molecular mechanisms for a presumed field cancerization within a Barrett’s esophagus, which has been discussed in the literature, however, remain elusive.

