











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
A 38-year-old man presented with dysphagia for solids fluctuating in severity. This symptom had persisted for several years. He reported feeling worse in the previous month, having also lost 10% of total weight. He had no relevant past medical history and physical exam was normal. Initial workup by upper endoscopy was normal. High-resolution esophageal manometry excluded outflow obstruction of the esophagogastric junction or peristalsis disorders but identified a horizontal and pulsatile high-pressure area below the upper esophageal sphincter (Fig. 1a, b, see arrows). The initial interpretation of the manometry, as the high-pressure area maintained itself throughout the exam, gave rise to the search for an extrinsic cause. Barium swallow was then performed, revealing an extrinsic compression at the level between the upper and middle thirds of the esophagus (Fig. 2a, b, see arrows). A thoracic computed tomography angiography identified an abnormal origin to the right subclavian artery, after the left subclavian origin (Fig. 3, see arrow).
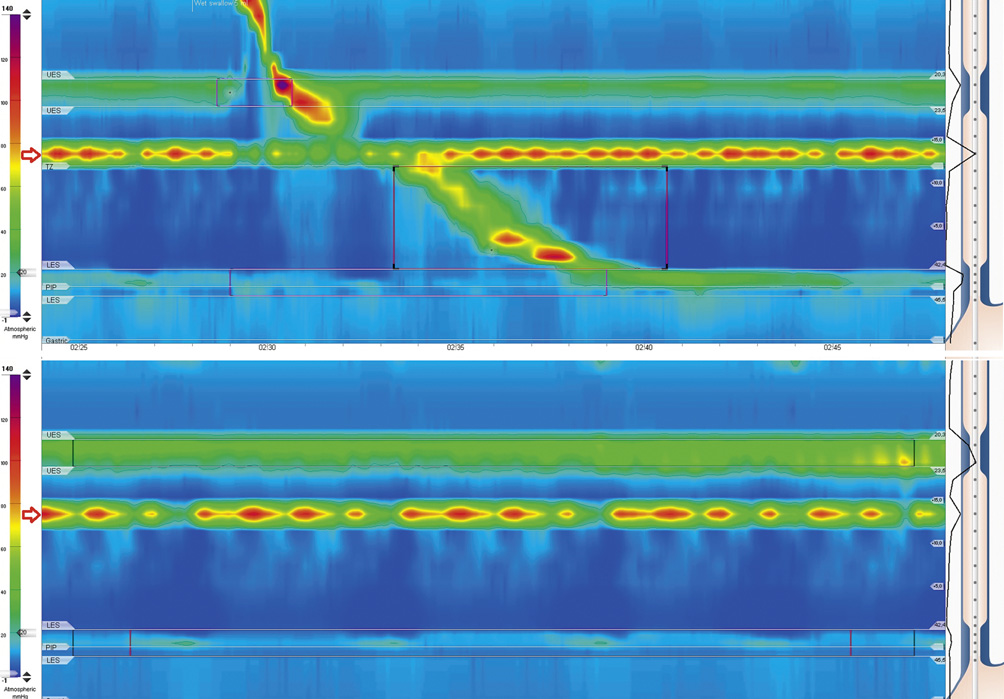
Fig. 1 a, b High-resolution esophageal manometry: a horizontal high-pressure area is pictured just beneath the upper esophageal sphincter.
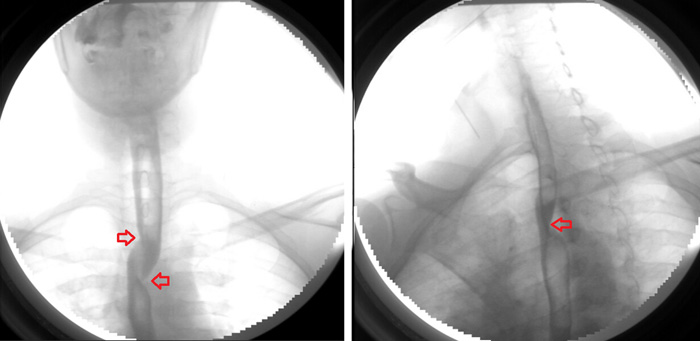
Fig. 2 a, b Barium swallow: an extrinsic compression can be seen, as pointed out by the red arrows, between the upper and middle thirds of the esophagus.
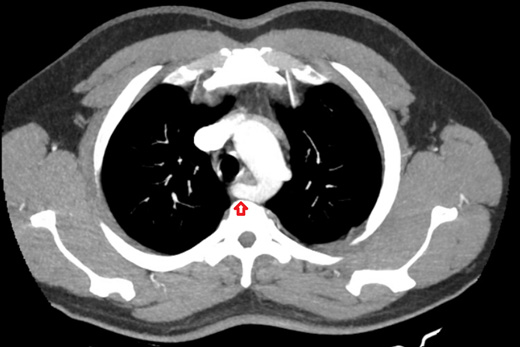
Fig. 3 Due to suspected dysphagia lusoria, the patient underwent thoracic computed tomography angiography confirming an abnormal origin to the right subclavian artery (see arrow).
The patient refused surgical intervention and maintains mild symptoms under general measures. The abnormal right subclavian artery, also known as the arteria lusoria, is present in 0.5-2.5% of the general population and causes symptoms in about 20% [1, 2]. Despite being congenital, it leads todysphagia morefrequently after the 5th decade of life [2]. The present case intends to raise awareness to the potential role of high-resolution manometry in the diagnosis of this rare condition.

