











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkA 71-year-old woman was referred for treatment of a sessile polyp (0-Is) in the sigmoid described as having altered crypt morphology and disrupted vascular pattern on virtual chromoendoscopy, indicative of malignancy. The endoscopic biopsies revealed no dysplasia.
We repeated colonoscopy, and a sessile polypoid lesion (0-Is) adjacent to a diverticulum with a large ostium was identified. The polyp had a pale color and a small ulceration on white-light endoscopy, measuring 12 mm (Fig. 1). Narrow Band Imaging (NBI) assessment revealed the absence of pit pattern and an aberrant vascular pattern with dilated, irregular, tortuous vessels (Fig. 2). Histological assessment (several biopsies) of the lesion revealed polypoid granulation tissue with fibrinoid necrosis, suggestive of ulceration (Fig. 3). The diagnosis of granulation polypoid tissue arising from a colonic diverticulum was established, and due to its benign nature, we decided not to remove it.
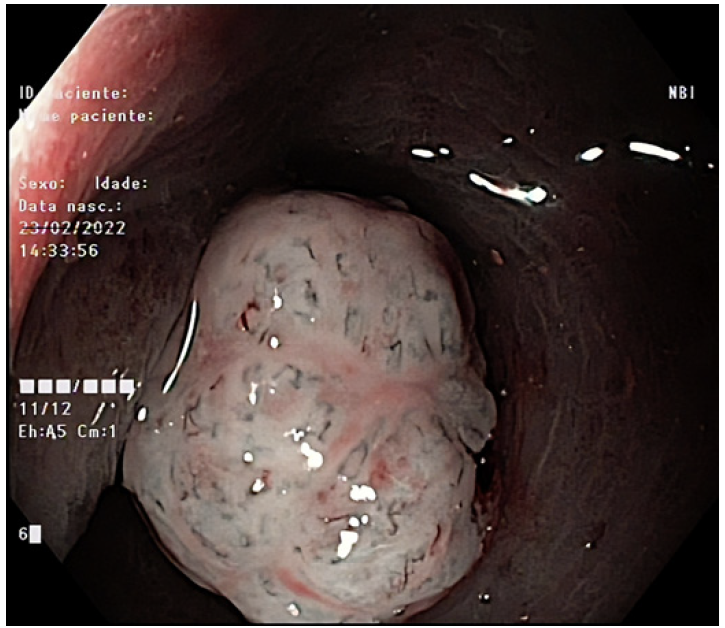
Fig. 1 Sessile polyp (0-Is) with approximately 12 mm located in the sigmoid. It has a pale color and aberrant vessels.
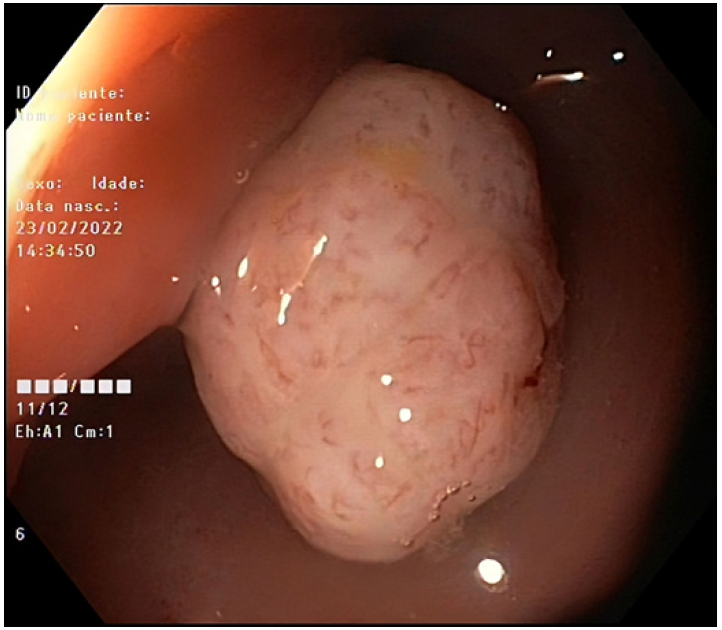
Fig. 2 Narrow band image (NBI) evaluation of the 12 mm sessile polyp, revealing the absence of glandular pattern with aberrant vessels, without evidence of adenomatous tissue.
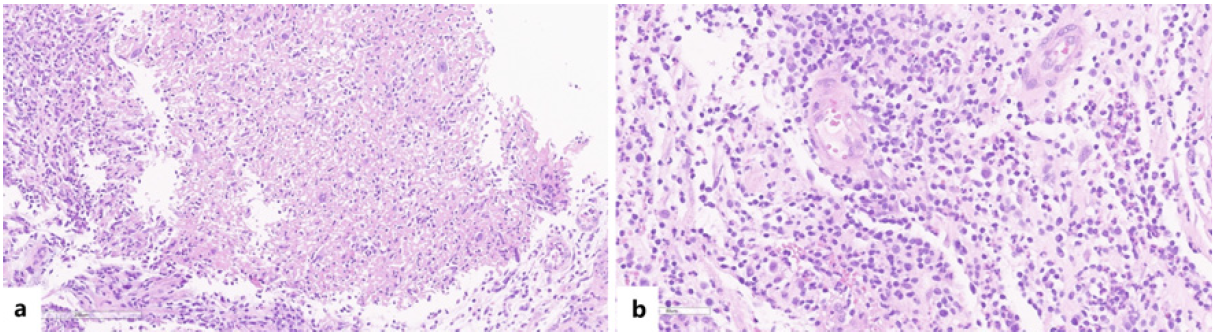
Fig. 3 a Histological findings of biopsies of the polyp. A 10 magnified image with a hematoxylin and eosin (HE) stain, where the blue line reveals fibrinoid necrosis, typical of ulceration. No atypical cells or structural atypia. b Histological findings of biopsies of the polyp. A 20 magnified image with a hematoxylin and eosin (HE) stain, which reveals increased outgrowth of microvascular structures and infiltration of lymphocytes, neutrophils, and plasma cells, which indicates granulation tissue. No atypical cells or structural atypia.
Granulation polypoid tissue is a rare entity with, to our knowledge, just a few case reports on the literature [1-3]. Granulation polypoid tissue could arise from a colon diverticulum after recurrent diverticulitis and has no malignant potential, contrary to neoplasms.
These polyps are composed by inflamed granulation tissue and covered by regenerative epithelium and not by colonic epithelium, so there are no crypts on the surface [3]. Subsequently, on virtual chromoendoscopy, they have a fibrotic appearance without pit structures, which could be misinterpreted as the amorphous appearance that characterizes invasive neoplasia [1-4]. In order to differentiate these entities, one should search for other features of neoplasms, despite being nonspecific. Theseinclude the presence of an adenomatous component at the periphery or extensive ulceration and friability [4]. Although further investigation is required, according to the similarity of endoscopic images described in the available literature [1-4], we thus speculate that a colonic polyp showing a smooth surface, lack of pit structure, a fibrotic appearance, and aberrant neo-vessels may be typical of a colonic granulation polyp.

