











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Inflammatory bowel disease (IBD) includes both Crohn’s disease (CD) and ulcerative colitis (UC). IBD is a worldwide burdensome chronic inflammatory disease of the gastrointestinal tract [1] with a significant impact on patient’s quality of life [2]. Nowadays, patient-reported outcomes (PROs) are considered an important tool for personalized clinical management [3], and it is advised to assess PROs early and frequently during IBD course [4]. Patients with IBD often believe diet to have a symptom-triggering role [5-7], which can not only lead to maladaptive dietary modifications but may also affect patients’ psychological and social well-being [7]. Recently, food-related quality of life (FR-QoL), which measures dietary restrictions and daily life limitations driven by eating and drinking [8, 9], has been acknowledged as an important PRO in IBD [4]. Indeed, FR-QoL has been shown to be significantly impaired in IBD [9]. However, this is still not routinely assessed by IBD clinicians, neither in clinical practice nor in research. Recently, a FR-QoL questionnaire was developed [5], following qualitative interviews with patients with IBD [8]. This instrument was designed to systematically measure the psychosocial factors surrounding eating and drinking in IBD. Afterward, the FR-QoL-29 questionnaire has been used in different English-speaking countries to show impaired FR-QoL in patients with IBD, both in adults [10-12] and in children [13]. Moreover, this instrument was shown to be valid and reliable for assessing FR-QoL in culturally diverse English-speaking populations (e.g., Hispanics and Caucasians) [14], and there is already a validated translation of the FR-QoL to the Turkish language [15]. To the authors’ knowledge, no validated translation to the Portuguese language has been performed. To adequately use the FR-QoL questionnaire in a Portuguese-speaking population, adaptation and validation of a translated version were necessary. We aimed to translate and validate a Portuguese version of the FR-QoL-29 (FR-QoL-29-Portuguese) and to evaluate its reliability, validity, and responsiveness, to assess dietary restrictions and daily life limitations driven by eating and drinking in Portuguese patients with IBD.
Materials and Methods
The FR-QoL Questionnaire
As stressed, the FR-QoL questionnaire addresses the eating and drinking experience of IBD patients. The questions revolve around the feelings and thoughts patients with IBD have around buying and preparing food, and how it affects their lifestyle and social commitments. This includes enjoyment of food, dietary restrictions, social eating situations, and the psychological impact of managing a diet under the constraints of IBD. The questionnaire also addresses fear of food-triggered symptoms, aiming to provide comprehensive insights into the intersection of diet, social life, and well-being in the context of IBD. This instrument has 29 questions measured on a five-point Likert scale. The sum score ranges from 29 to 145. A higher sum score indicates greater FR-QoL, and a lower sum score indicates a poorer FR-QoL. There are no validated cutoff values [8].
Translation and Adaptation of the FR-QoL to the Portuguese Language
After obtaining permission from the copyright holders (King’s College London), the FR-QoL-29 was translated to Portuguese following a thorough methodological approach [16-18]. The original version was independently translated into Portuguese by two bilingual investigators (R.O. and J.R). The research team compared and assessed the two translations for ambiguities or discrepancies between the original version and the forward translations. A single blind back translation to English was then performed by another bilingual investigator (H.T.S.), and this back translation was compared by the research team with the original version to ensure conceptual, semantic, and content equivalence between the source and target language versions. Subsequently, a convenience sample of 3 Portuguese IBD patients evaluated the pre-final version and made suggestions for improving clarity and ease of comprehension. Before the final discussion took place, the teams’ IBD expert (H.T.S.) evaluated each item of the questionnaire for content validity. Finally, a discussion between the research team took place to reformulate some items according to the cognitive debriefing of the patients and the expert’s revision, and a final translated version (FR-QoL-29-Portuguese) was reached.
Study Design
To perform this validation study, the authors conducted a cross-sectional case-control study to assess differences regarding FR-QoL between a Portuguese IBD population and a control population (patients referred to a Gastroenterology appointment for in-hospital colorectal polypectomies and hospital volunteer blood donors) [19]. Briefly, this was a survey-based study using a multimodal questionnaire that assessed both demographic and clinical data, patients’ disease-related QoL and FR-QoL. This study was conducted in a Portuguese tertiary hospital (Algarve Uni-versity Hospital Centre) between May and July 2022. All outpatient adult IBD patients were invited to participate, as long as they were native Portuguese speakers willing to provide consent, were not receiving parenteral or enteral nutrition, and were not pregnant or breastfeeding.
Participation rate was defined by the ratio of patients who were invited to participate in the study and agreed to do so. Completeness rate was defined as the ratio of participants who completed all the questions of the survey. If more than 20% of answers were missing from a questionnaire, that questionnaire was excluded.
The necessary sample size for any study is dependent on the individual characteristics of the study, and there are no clear guidelines on the ideal sample size for validation studies [20]. Despite this, based on the available literature, we considered a minimum respondent-to-item ratio of 5:1 [18, 21]. Therefore, a minimum of 145 participants would be required to adequately assess the operational properties of the 29-item scale. Allowing for potential dropouts or missing data, and since a larger sample size allows for better quality of psychometric testing, we used a consecutive sample of IBD patients, granting a minimum of 145 patients would be reached.
Patients were asked to complete the FR-QoL at a first timepoint and at a second timepoint 4 weeks later. Additionally, at this first timepoint, demographic and clinical data were collected (sex, age, disease type, disease duration, current medication, history of IBD-related surgery, latest inflammatory biomarker [faecal calprotectin], Harvey-Bradshaw index [HBI] for CD and partial Mayo score [pMS] for UC, patients’ body mass index, smoking status, history of nutritional counselling), and patients would also fulfil the Short Inflammatory Bowel Disease Questionnaire (SIBDQ) to assess disease-related QoL [22]. At the second timepoint, the patients were also questioned about whether they felt their general well-being to be “similar, better, or worse” than at baseline. Controls were asked to complete the FR-QoL only once, during outpatient appointments, and simple demographic data were collected (sex, age).
Ethical Considerations
The study conforms to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the Algarve University Hospital Centre Administration Board (April 21, 2022) and Research Ethics Committee (April 7, 2022). Written, informed consent was obtained from all patients by one of the investigators after explaining the aims of the present study.
Statistical Analysis Reliability
Reliability measures the consistency of the survey results. This property was ensured by the questionnaire internal consistency and test-retest reliability. Internal consistency reflects the extent to which the different items of a questionnaire measure the same construct. It was assessed using Cronbach’s α coefficient [16]. Test-retest reliability refers to the extent to which individuals’ responses to questionnaire items remain relatively stable over time [18]. It was assessed using the intraclass correlation coefficient [23]. An interval of 4 weeks was considered long enough to prevent recall bias. Only patients who reported to maintain the same general well-being as at baseline were used in this analysis to guarantee similar disease status.
Validity
Validity determines whether the questionnaire measures what it was in fact designed to measure [18]. Content validity, which evaluates if the questionnaire items are representative of the theoretical construct that the questionnaire assesses [18], was ensured by an each-item throughout analysis by an IBD expert (H.T.S.) after the final translation, as previously described.
Construct validity was measured through convergent and discriminant validity [18] and hypothesis testing [16]. We hypothesised that the FR-QoL-29-Portuguese overall score would positively correlate with the SIBDQ-PT and negatively correlate with patients’ disease activity, as measured by HBI or pMS (symptom-based scores), and faecal calprotectin (inflammatory biomarker). We also hypothesised that having IBD and current disease activity would be associated with lower FR-QoL-29-Portuguese scores, compared with controls and patients with inactive disease. For correlation analysis, Spearman’s correlation coefficient was calculated.
Active disease was defined through a HBI ≥5 or a pMS ≥2 [24], and faecal calprotectin above 250 μg/g [4], when a recent (2-month timeframe) faecal calprotectin was available. Disease was considered to be in remission when patients had an HBI <5ora pMS <2 [24], and faecal calprotectin below 250 μg/g. When faecal calprotectin was unavailable within the predefined timeframe, only symptom-based scores were considered to define disease activity.
Responsiveness
Responsiveness measures the extent to which a questionnaire can detect changes over time in the construct being measured [18]. A Wilcoxon test was used to compare the median overall scores of FR-QoL-29-Portuguese between the first and the second timepoints. According to patients’ responses regarding general well-being modifications, three groups of patients were defined: those who referred “an overall worsening of general well-being,” those who referred “an overall improvement of general well-being,” and those who reported to have “similar general well-being,” compared to baseline. A p < 0.05 was considered statistically significant.
Results
FR-QoL-29 Translation and Cultural Adaptation The FR-QoL-29 was translated to Portuguese following a thorough and multiphase process, which included forward translation, reconciliation, blind back-translation, forward and back translation harmonization, comprehensibility assessment by a sample of Portuguese IBD patients, and item per item content validity judgement by a bilingual IBD expert. Finally, the research team discussed the results of the patients’ cognitive debriefing and the expert’s evaluation, and a final translated version of the questionnaire was reached and proofread.
During the forward and back translation process, minor discrepancies regarding sentence structure and use of synonyms were found and reconciled. Importantly, one major issue concerning the five Likert-scale response options was identified and clarified after a research team meeting. In detail, the first and last Likert-scale response options in the original version are “strongly agree” and “strongly disagree,” which would be translated to Por-tuguese as “concordo fortemente” and “discordo fortemente,” respectively. However, because the alternatives “concordo totalmente” and “discordo totalmente” (“totally agree” and “totally disagree,” respectively) are more commonly used in Portuguese, those were chosen for the final version, ensuring semantic equivalence.
Both the patients’ cognitive debriefing and the expert’s evaluation raised concerns about the comprehensibility of the verb tenses used. In fact, the original version has many items written in the present perfect continuous, which is not typically used in spoken Portuguese. As such, to improve the ease of quaestionary comprehensibility, the simple past was chosen as the preferred verb tense.
Regarding content equivalence, the IBD expert considered all items to be either “relevant but needing minor alterations” (namely, the verb tense in use, as explained) or “very relevant and succinct.” As so, the questionnaire was considered to have acceptable content-related validity by the expert involved. Lastly, the final version was approved by the original authors of the instrument. The licence to use the FR-QoL-29-Portuguese can be obtained from kevin.whelan@kcl.ac.uk.
Sociodemographic and Clinical Data and Score Results
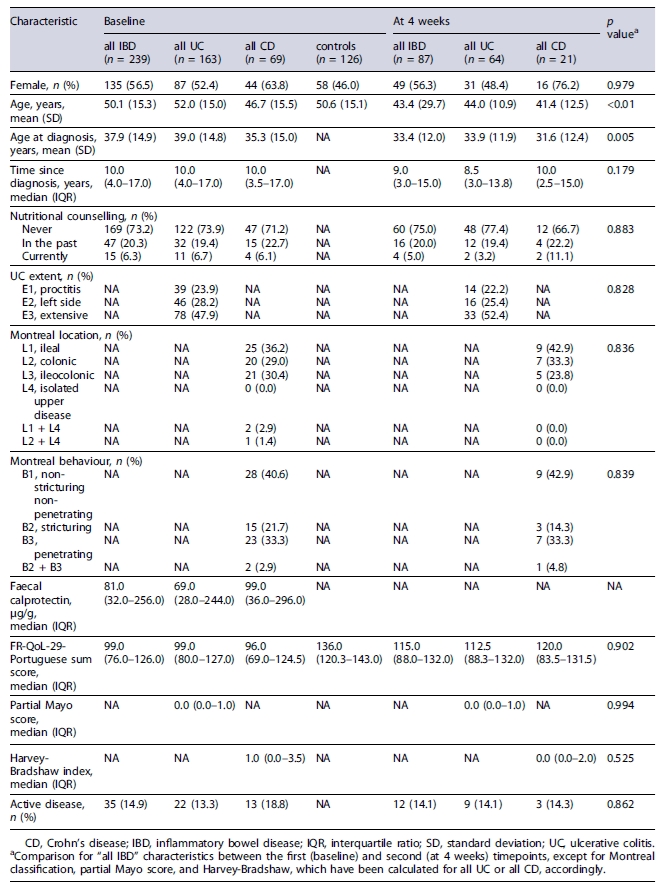
Two-hundred thirty-nine patients with IBD and 126 ontrols were included in the study and fulfilled the FR-QoL Portuguese at the first timepoint. The participation rate for IBD patients was 99.6% and the questionnaire completion rate was 100%. Only 1 patient declined to participate in the study as he claimed not to consider it relevant to his situation. As so, all handed questionnaires were complete and included in the analysis. Overall, age and gender were similar between IBD patients and controls. Patients and controls’ demographic data, and patients’ clinical characteristics are described in Table 1. Faecal calprotectin values were available for 175 (73.2%) of the patients. FR-QoL-29-Portuguese scores were significantly lower for IBD patients than controls (median 99.0 [IQR 76.0-126.0] vs. 136.0 [IQR 102.8-143.0]; p < 0.001).
At the second timepoint, 87 (36.4%) patients answered the questionnaire. Sex and patients’ clinical characteristics were comparable between timepoints, except for age, which was higher at baseline (Table 1). The median FR-QoL-29 Portuguese scores at the first and second time-point were 99.0 and 115.0 (IQR 76.0-126.0 and 88.0-132.0; p = 0.902) (Table 1).
Reliability
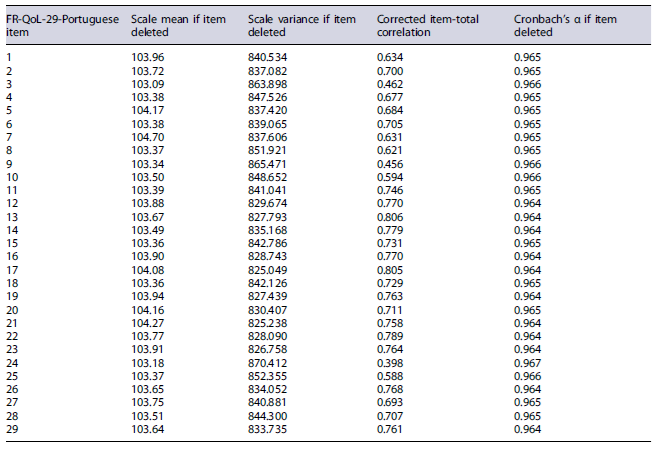
The FR-QoL-29-Portuguese Cronbach’s α coefficient was 0.966, indicating excellent internal consistency. Moreover, Cronbach’s α coefficient did not significantly improve when items were eliminated one by one, and as such, there was no need to consider eliminating any item of the questionnaire (Table 2). Furthermore, the test-retest reliability revealed a good temporal stability of the FR-Qol-29-Portuguese between the baseline and the second timepoints, considering an intraclass correlation coefficient of 0.767 (95% CI: 0.644-0.848).
Validity
We had a priori hypothesised that FR-QoL-29-Portuguese would positively correlate with SIBDQ-PT and negatively correlate with disease activity. These hypotheses were confirmed, as a positive moderate correlation between FR-QoL-29-Portuguese and SIBDQ-PT scores (R = 0.490, p < 0.001), and a negative correlation between FR-QoL-29-Portuguese and disease activity symptom-based scores (R = −0.277 for UC, R = −0.388 for CD; p < 0.001) and faecal calprotectin were found (R = −0.150, p = 0.041).
As for questionnaire discriminant validity, patients with IBD scored lower than controls (all IBD: median 99.0 [IQR 76.0-126.0] vs. controls: 136.0 [IQR 102.8-143.0]; p < 0.001), and patients with active disease scored lower than patients with inactive disease (active: median 80.0 [IQR 56.0-99.0] vs. inactive: 103.5 [IQR 81.0-128.8]; p < 0.001).
Responsiveness
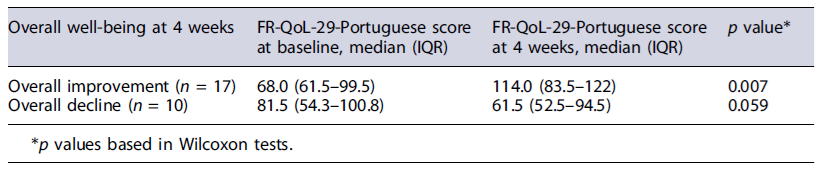
Out of the 87 patients who fulfilled the FR-QoL-29-Portuguese at the second timepoint, 17 (19.5%) reported an “overall improvement of well-being.” For these patients, the median sum score on FR-QoL-29-Portuguese was significantly higher than at baseline (114.0 vs. 68.0; p = 0.007). A median improvement of 15.0 points (IQR 3-0.48.5) was detected. For the 10 (11.5%) patients who reported an “overall decline of well-being,” themediansumscoreonFR-QoL-29-Portuguese was lower than at baseline, though this difference was not statistically significant (61.5 vs. 81.5; p = 0.059). Still, a mean decline of 12.0 points (IQR 23.5-3.5) was observed (Table 3).
Discussion
In this study, we present a translation to the Portuguese language of the FR-QoL-29, after independent forward and back translations, as well as assessment for content and semantic equivalence by both an IBD expert and an IBD patient group. The FR-QoL-29-Portuguese was applied to a Portuguese IBD sample at two time-points to confirm the questionnaire reliability, validity, and responsiveness to change.
Two-hundred thirty-nine and 87 patients with IBD answered the questionnaire at the first and second timepoint, respectively. Despite the observed drop in response rate between the first and second timepoints, this panel size is in line with previous studies [8, 15] and was considered to be appropriate to evaluate all FR-QoL-29-Portuguese psychometric properties.
The FR-QoL-29-Portuguese showed excellent internal consistency (Cronbach’s α value of 0.966). Likewise, the validation studies of the original English FR-QoL-29 tool and the FR-QoL-29-Turkish showed similar properties with aCronbach’s α of 0.959 [8] and 0.96 [15], respectively. Furthermore, the correlation coefficients between individual items and the total sum score of the FR-QoL-29-Portuguese ranged from 0.398 to 0.806, and Cronbach α coefficient did not significantly improve when items were eliminated one by one. As such, the Portuguese version of the FR-QoL-29 has the same items as the original version of the instrument. Lastly, test-retest reliability showed good temporal stability at a 4-week interval. Overall, these measures establish the FR-QoL-29-Portuguese to be a highly reliable tool to measure FR-QoL in the Portuguese population.
The FR-QoL-29-Portuguese construct validity was demonstrated through the confirmation of a priori formulated hypothesis: the FR-QoL-29-Portuguese sum score correlated positively with SIBDQ-PT and negatively with disease activity surrogates (symptom-based scores and faecal calprotectin). In fact, FR-QoL has previously been shown to correlate with disease-specific QoL in IBD [8], and patients with higher symptom burden and clinical activity have been reported tohave poorerFR-QoL [8,10,12,15].Additionally, patients with IBD had significantly lower scores than controls without IBD, demonstrating an excellent discriminant validity of the questionnaire, similar to the original version [8]. Interestingly, in our cohort, both IBD patients and controls reported higher FR-QoL-29 scores than those in other studies [8-10, 12]. Sixty percent of patients scored the maximum points (“totally agree”) in question number 24, which concerns feeling comfortable about eating and drinking around people despite their IBD. In the Portuguese culture, it is very common for eating and drinking to occur in a social context, such as at parties, events, and even in the workplace. The tradition of sharing meals and drinks with family, friends, and colleagues is deeply rooted in Portuguese culture. As such, we may elaborate that the importance placed on these social moments around the table may at least partially explain why Portuguese people scored higher in FR-QoL questionnaires.
The participation rate for IBD patients in this study on FR-QoL was 99.6%, and the questionnaire completion rate was 100%. These results suggest that our IBD population is highly interested in discussing these issues. This tool could be applied during initial evaluations and follow-ups, especially for patients concerned with diet management, those altering their lifestyle due to IBD, or those considering nutritional counselling. This approach would underscore the importance of addressing diet-related issues in clinical practice, despite time constraints during appointments.
This study has several strengths that ought to be highlighted. We recruited a large sample, representative of the outpatient population across all stages of disease, in terms of phenotype, disease activity, and duration. Besides, the case-control design allowed to evaluate the discriminant validity of the Portuguese questionnaire. To our knowledge, this is the first study showing that FR-QoL-29 is responsive to changes in overall well-being, further supporting its role as an important tool to measure FR-QoL in IBD. Nevertheless, the study may have been underpowered to detect responsiveness to an overall decline in well-being, and further validation of responsiveness should be carried out in a larger sample. Moreover, this was a unicentric study, although this sample size allowed complete psychometric assessment of the instrument’s properties. Lastly, because we did not have the possibility of using an expert panel, content validity index could not be calculated, and as such, content validity was based on the evaluation of a single IBD expert.
In conclusion, the FR-QoL-29-Portuguese is a valid and reliable tool to evaluate FR-QoL in Portuguese patients with IBD. It is convergent with health-related QoL and disease activity surrogates and responsive to change, highlighting its value in both clinical practice and research.

