











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Autoimmune gastritis (AIG) is a chronic, inflammatory disease characterized by progressive atrophy - with or without intestinal metaplasia - and enterochromaffin like cell hyperplasia of gastric oxyntic mucosa (acid-secreting gastric compartment), sparing the antral mucosa [1, 2]. This condition increases the risk of both neuro-endocrine tumours and cancer development in the stomach [3-5]. AIG is usually suspected when either iron or B12 deficiency anaemia develops, due to the reduction of gastric acid and intrinsic factor secretion, respectively [6]. Moreover, it is searched for at endoscopy in patients with positive serology to parietal cell autoantibodies, generally screened in patients with other autoimmune diseases, such as autoimmune thyroiditis or type 1 diabetes mellitus [6]. However, some patients with AIG complain of dyspeptic or even gastro-oesophageal reflux symptoms, so AIG may be also diagnosed at gastric biopsies performed during routine endoscopy [7]. According to current guidelines, standard sampling of gastric mucosa should be accomplished in 90% of ap-propriate upper endoscopies to search for Helicobacter pylori infection and gastric precancerous lesions, that is, atrophy and intestinal metaplasia, including AIG [8, 9]. However, these conditions are present in only a minority of patients with normal-appearing gastric mucosa, so the histological results are often clinically unrewarding. Indeed, an AIG prevalence as low as 1.9% was reported in a serology study in the USA [10], and 2.7% in three large endoscopic series from Italy, Australia, and Tunisia [11-13].
The interest towards gastric juice analysis during routine endoscopy has been renewed by the marketing of EndoFaster®, a device that performs a real-time evaluation of both ammonium and H+ concentrations in the gastric juice, allowing to accurately rule out H. pylori and extensive atrophy involving antral and gastric body mucosa [14, 15]. Indeed, negative predictive values of gastric juice analysis as high as 97% on more than 2,000 patients were reported in a recent systematic review [16]. However, no specific data on EndoFaster® performance in AIG patients are available. Therefore, we designed this study to assess whether gastric juice analysis allows ac-curate exclusion of the presence of AIG in real time so that gastric mucosa sampling on normal-appearing mucosa may be safely and conveniently avoided.
Materials and Methods
Patients
This retrospective study was performed on data prospectively collected in a specific database where information of consecutive adult patients who underwent gastric juice analysis at upper endoscopy was registered. For this study, data of all patients diagnosed with AIG were retrieved and compared to those of matched controls enrolled in the same database. Inclusion criteria were (a) histologically proven AIG;(b) no use of proton pump inhibitor therapy in the last 2 weeks before endoscopy; (c) absence of H. pylori at histology; (d) no previous therapy for H. pylori infection. These criteria were adopted to appropriately exclude present or past H. pylori infection potentially triggering atrophy/intestinal metaplasia development on gastric mucosa, in order to study only patients with true AIG. For each case, data of 5 controls matched for gender and age (±2 years) and with the same inclusion criteria, but without AIG, were recovered.
Endoscopic Procedures
All patients underwent upper endoscopy with standard (2 antral, 1 incisura angularis, 2 gastric body) biopsies on gastric mucosa, according to the updated Sydney system [17]. AIG was diagnosed when glandular atrophy (with or without intestinal metaplasia) with enterochromaffin-like cell hyperplasia was confined to the oxyntic mucosa, and a feature of normal antral mucosa was confirmed at histology [1]. During endoscopy, gastric juice analysis was performed by EndoFaster® (manufacturer: NISO Biomed S.r.l, Turin, Italy; distributor: Waldner Tecnologie Medicali, Trento, Italy). In detail, the device was interposed between the endoscope and the suction system, without causing any discomfort to the patient (Fig. 1). During endoscopy, lumen washing was avoided until the stomach was reached and at least 3 mL of gastric juice was aspirated. The device performs a real-time (within 90 s) gastric juice evaluation of pH values and ammonium concentrations, to suspect atrophic gastritis and H. pylori infection, respectively [16]. A threshold of pH less than 4.5 was adopted as cut-off to rule out the presence of atrophy involving the oxyntic mucosa and, then, a feature of AIG [16]. Informed consent was obtained for all the procedures. Since no identification of patients was allowed, no experimental drugs were administered, no additional costs or procedures for the patients were required, and no funds were received, the Investigational Review Boards waived formal approval for this retrospective analysis on medical records.

Statistical Analysis
Frequencies, percentages, and mean values with their 95% confidence intervals were calculated for all observations. Sensitivity, specificity, positive predictive value, negative predictive value (NPV), accuracy, positive likelihood ratio, and negative likelihood ratio were calculated, and Fagan’s nomogram accordingly was designed.
Results
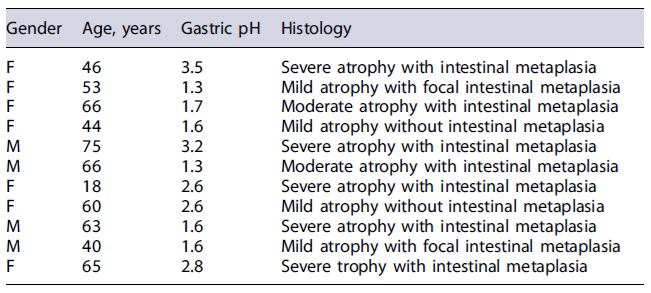
Overall, data of 40 patients (M/F: 19/21; mean age: 58 years, range: 18-89) diagnosed with AIG and 212 matched (102/120; mean age: 59 years, range: 19-92) controls were evaluated. Among AIG patients, the feature of atrophy/metaplasia on the oxyntic mucosa was staged as severe in 22 (55%) cases, moderate in 9 (22.5%), and mild in the remaining 9 (22.5%) patients. Gastric juice analysis showed a pH value >4.5 in 29 (72.5%) patients and 12 (5.7%) controls. Sensitivity, specificity, positive predictive value, NPV, and the overall accuracy were 73% (95% CI = 0.57-0.84), 94% (95%CI = 0.90-0.97), 71% (95% CI = 0.64-0.74), 95% (95% CI = 0.93-0.97), and 91% (95% CI = 0.87-0.95), respectively, while the positive likelihood ratio value was 12.9 (95% CI = 7.19-23.03), and the negative likelihood ratio was 0.29 (95%CI = 0.18-0.48). Distribution of patients according to EndoFaster® results and AIG feature is provided in Table 1, and Fagan’s nomogram in Figure 2 [2]. Data regarding the 11 false-negative cases are provided in Table 2. As shown, the histological assessment showed the presence of mild-moderate atrophy of oxyntic mucosa in 6 (54.5%) cases, and severe in the remaining 5 cases.
Table 1. Distribution of patients based on EndoFaster results (positive when pH >4.5) and histological feature of autoimmune gastritis (AIG)
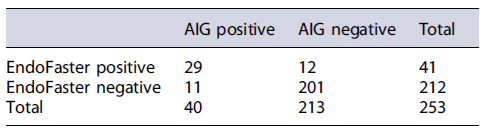
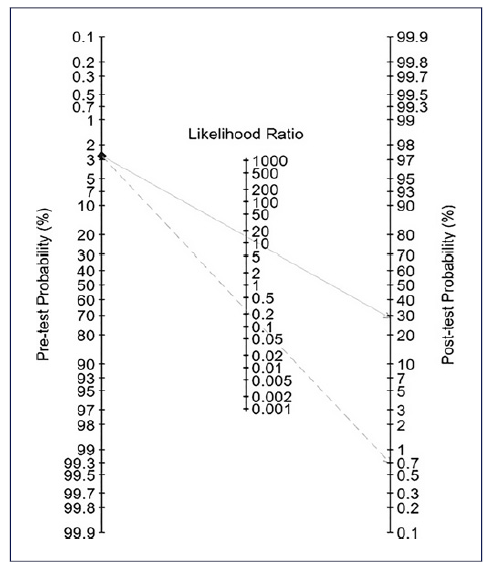
Fig. 2. Fagan’s nomogram. The pretest probability indicated in the nomogram was that calculated in endoscopic studies.
Discussion
Upper endoscopy is largely performed in routine practice for diagnostic, therapeutic, and follow-up purposes [9, 18]. However, the rate of inappropriate examinations in open-access setting was >20%, with values reaching 61.7% in some series [19]. According to current guidelines, standard gastric biopsies should be performed during routine endoscopy to search for both H. pylori infection and precancerous lesions on gastric mucosa, namely atrophy and intestinal metaplasia [8, 9]. AIG, characterized by atrophy and/or metaplasia confined in the oxyntic mucosa of the stomach and increased risk of developing both type I NET and adenocarcinoma in the stomach [1, 2], is a quite infrequent condition. Indeed, a prevalence rate of less than 3% was reported in endoscopic studies performed in different geographic areas [11-13], and ranging between 3% and 9% in serological studies only on Scandinavian populations where the incidence of disease is particularly high [6].
Although generally suspected in patients with anaemia (micro- or macrocytic) or with parietal cell autoantibody seropositivity, AIG may be unexpectedly detected at histological assessment of gastric mucosa of patients with dyspepsia, particularly subtype post-prandial distress syndrome or even with gastro-oesophageal reflux symptoms [7]. Can the gastric juice analysis be useful to avoid useless biopsies on normal-appearing mucosa without missing AIG? To achieve this purpose, a test with a very high NPV is needed. Real-time pH measurement in gastric juice with EndoFaster® was found to accurately rule out the presence of extensive atrophy/metaplasia involving both antral and gastric body mucosa [16]. To our knowledge, this is the first study on the accuracy of such a device in AIG patients. Our data found that by performing gastric juice analysis it is possible to rule out the presence of AIG with an NPV as high as 95%, so that only 5 patients in every 100 cases with negative EndoFaster® testing would be eventually overlooked for AIG. Of note, we observed that only mild-moderate atrophy on the oxyntic mucosa was present in more than half of patients with false-negative results at pH measurement. Therefore, it could be speculated that the patchy reduction of appropriate acid-secreting gastric glands revealed at histological assessment could be insufficient to markedly impair acid secretion detectable by pH measurement. On the other hand, the diagnosis of mild atrophy on gastric mucosa could represent an over-reporting, when considering that gastric biopsy specimens are not routinely oriented in clinical practice [20] and that interobserver agreement for atrophic gastritis among expertpathologistsisonly 0.73 [21]. Therefore, an even better performance of EndoFaster® in this setting could be foreseeable. On the other hand, beyond reducing useless biopsies in a negative test, a positive EndoFaster® result would alert the endoscopist to take standard biopsies on antral and gastric body mucosa. Indeed, despite it is recommended that gastric biopsies should be taken in >90%of endoscopies [8, 9, 22], the routine biopsy rate was quoted as low as 23% in a recent Italian study [23].
In the past, a pH 4 cut-off was proposed to rule out atrophy/metaplasia involving gastric oxyntic mucosa, because only few patients with this histological condition showed a pH value of gastric juice lower than 4 [24, 25]. However, a pH 4.5 cut-off was adopted in successive studies to disclose severe hypochlorhydria due to diffuse atrophy on gastric mucosa and, therefore, we cautionarily used the latter cut-off to rule out AIG [14, 15, 26].
Besides pH measurement, gastric juice analysis with EndoFaster® was found to be highly accurate in simultaneously excluding H. pylori - namely a type I carcinogen for gastric cancer according to the IARC [27]- by assessing ammonium concentration [16]. Therefore, it is clearly evident the advantage in contemporary discarding H. pylori infection and precancerous lesions by real-time gastric juice analysis with EndoFaster®. Moreover, avoiding foreseeable negative gastric biopsies in a definite portion of patients through the gastric juice analysis was found to distinctly reduce the environmental impact of upper endoscopy [28].
Some limitations of the study should be considered. The sample size is quite small, so our findings need to be confirmed in a larger, multicentre study. Although a standard biopsy sampling is routinely performed in our centre, the retrospective design of the study prevents specifically verification of the quality of endoscopic procedures or biopsies protocol in all cases. Finally, we excluded subjects with ongoing PPI use or presence of H. pylori infection, two conditions quite frequently encountered in routine practice.

