











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkA 79-year-old diabetic woman presented at the emergency room with fever, retrosternal pain, and dysphagia 24 h after choking on pork meat. A chest CT scan without oral contrast revealed a 2 cm dense linear structure crossing the thoracic esophageal wall, with signs of pneumomediastinum and densification of the periesophageal tissues (shown in Fig. 1) - these findings were compatible with mediastinitis due to esophageal perforation by bone.
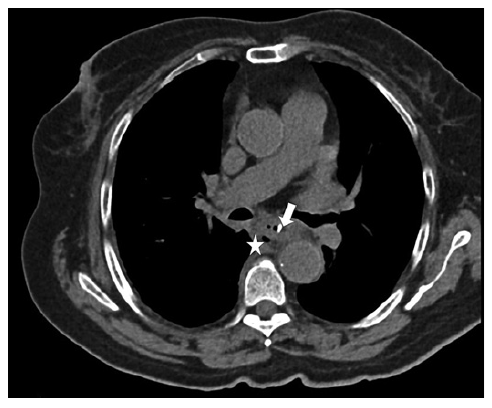
Fig. 1. Axial CT scan of admission showing the 2 cm linear structure crossing the thoracic esophageal wall (arrow) causing densification of periesophageal tissues and signs of pneumomediastinum (star).
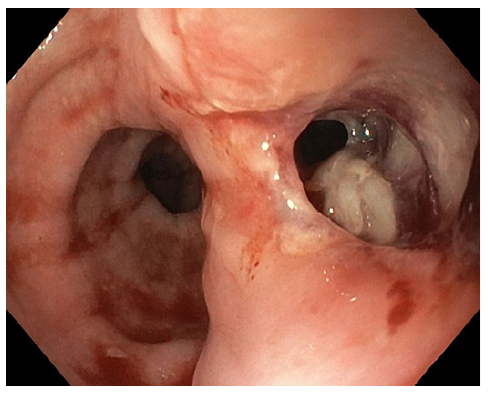
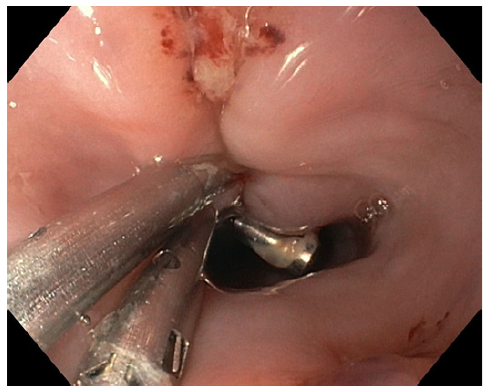
Upper digestive endoscopy was performed, with CO2 insufflation in the operating room in the presence of the general surgery team, under orotracheal intu-bation, and it identified a bone perforation 23 cm from the upper dental arch - the bone was removed with forceps only after unlocking and deflating the endotracheal tube cuff due to space conflict. After extracting the bone, a 15 mm esophageal perforation (shown in Fig. 2) was closed with 4 through-the-scope (TTS) clips (shown in Fig. 3).
It was decided to keep the patient intubated for 72 h; there was a good clinical and analytical evolution during this period. Afterward, a new CT scan was then performed, which showed successful closure of the esophagus, with no extravasation of oral contrast. She was then extubated without complications.
The patient underwent a 12-day nil-by-mouth regimen, under total parenteral nutrition, and 20 days of piperacillin/tazobactam + fluconazole, with good clinical and analytical response. A predischarge CT scan indicated resolution of the inflammatory process without oral contrast leakage.
Esophageal perforations are rare, with an incidence of 3.1 per 1,000,000 per year, but are associated with significant morbimortality [1]. Traditionally, surgery was the therapeutic modality of choice, but endoscopic management is now emerging as its first treatment modality [2, 3]. In the case of infracentimeter perforations, TTS clips can easily be used. In the case of larger perforations, other endoscopic options are primarily available, such as over-the-scope clips, stents, endoscopic suturing, or endoscopic vacuum therapy (when there is also need for infectious control) [1].
In this case, it was necessary to unblock and deflate the orotracheal tube cuff due to space conflict, in order to allow for the bone to be removed. Although the size of this
perforation was >10 mm, and attending to space conflict, closure with TTS clips was tried and successful - clinical judgment is always imperative. This case underscores the efficacy of endoscopic therapy for esophageal perforations and emphasizes the need for multidisciplinary involvement.

