











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Hepatocellular carcinoma (HCC) is the sixth-most common cancer worldwide and accounts for 90% of all primary liver cancers [1]. Over 90% of HCC cases occur in the setting of chronic liver disease, with cirrhosis from several etiologies as the primary risk factor. Hepatitis B virus (HBV) infection is documented in approximately 50% of HCC cases [2]. HCC metastasis can occur in different locations, with the most affected sites being the lungs, lymph nodes, and bones. Despite being a highly vascular tumor with intravascular dissemination, cardiac involvement is a rare manifestation (1-4%) and is usually diagnosed in patients with known HCC during oncology follow-up or as an autopsy finding [3].
Case Report
A 25-year-old male patient from Guinea, in Portugal for 6 months, with no known medical history presented with a 2-week history of fatigue, exertional dyspnea, anorexia, and weight loss. He also mentioned abdominal pain for the last 4 days. The patient consumed 20 g of alcohol per week and had no history of drug consumption or tobacco smoking habits. He was employed as a construction worker and did not have any relevant travel history. Physical examination showed a systolic murmur in the tricuspid area, an enlarged liver and right upper quadrant pain, with no ascites or signs of chronic liver disease stigmata. The electrocardiogram revealed sinus tachycardia with a right bundle branch block and the chest radiograph showed an enlarged cardiac silhouette. An echocardiogram showed an intracardial mass in the right atrium (RA) (80 mm × 64 mm), obstructing the tricuspid valve and causing functional stenosis. His laboratory tests showed normocytic anemia (hemoglobin 11.6 g/dL [ref. 13-17.5]), slightly elevated liver enzymes (AST 91 U/L [ref. 0-34], ALT 68 U/L [ref. 10-49], GGT 68 U/L [ref. 0-60], ALP 393 U/L [ref. 35-105]), with normal bilirubin (1.12 mg/dL [ref. <1.2]), and elevated NT-proBNP (457 pg/mL [ref. <300]). He underwent a computed tomography scan of the thorax, abdomen, and pelvis, which revealed multiple coalescent lesions evolving mainly the left and caudate lobes, consistent with multicentric HCC (shown in Fig. 1). Additionally, macrovascular invasion was observed in the left portal vein, middle suprahepatic veins, and inferior vena cava, extending into the lumen of the right ventricle and atrium. The intracardiac component measured 9 × 7.5 × 6 mm (AP ×T×L)(shown in Fig. 2). The computed tomography scan also identified bilateral pulmonary secondary lesions and signs of multiple segmental and sub-segmental bilateral pulmonary embolisms. Fur-ther investigation revealed an HBV infection (AgHbs positive, anti-Hbs negative, AgHbe positive, anti-Hbe negative) with a viral load of 1,160,000 IU/mL and an alpha-fetoprotein of 357,440 ng/mL (ref. <7). The patient was classified as Barcelona Clinic Liver Cancer (BCLC) Stage C due to the presence of extra-hepatic spread and portal invasion.
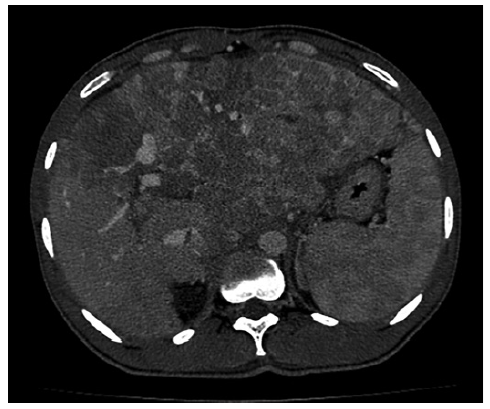
Fig. 1. CT scan of the abdomen. Heterogeneous hepatomegaly with multiple coalescent lesions involving most of the left and caudate lobes and also the right lobe, with arterial enhancement and washout, suggestive of multicentric HCC. CT, computed tomography.
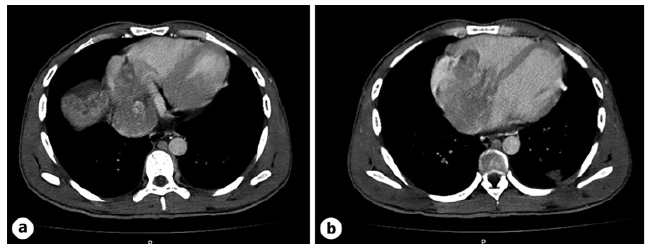
Fig. 2. CT scan of the thorax. a Macro-vascular invasion of the left portal vein, middle suprahepatic veins, and inferior vena cava. b Tumoral extension into the lumen of the right ventricle and atrium, with an intracardiac component measuring 9 × 7.5 × 6 mm (AP × T × L). CT, computed tomography.
After being discussed at a multidisciplinary team meeting, the patient was initiated on a regimen of tenofovir (300 mg/day) and sorafenib (400 mg/day). A few days later, the patient developed gastrointestinal side effects and stopped therapy. Due to rapid clinical and liver function deterioration, a palliative option was considered, and he died 1 month after the diagnosis of disease progression.
Conclusion
It is estimated that 854,000 new cases of HCC are diagnosed per year, with a growing incidence worldwide, making HCC a major global health problem [1]. In approximately 50% of HCC cases worldwide there is a subjacent HBV infection [2]. Although cirrhosis is considered the primary risk factor for HCC, chronic hepatitis B has carcinogenic potential itself by several mutagenetic routes, and up to 30% of chronic hepatitis B-related HCCs arise in non-cirrhotic liver, mainly in Asian patients, and patients with a family history of HCC. Therefore, HCC surveillance is recommended in European guidelines not only in cirrhotic patients but also in hepatitis B carriers with risk factors (family history of HCC or Asian patients over 40 or 50 years old, in men and women, respectively) [1]. On the other hand, in 2019, the burden of HBV infection was significant globally, with an estimated all-age prevalence of chronic HBV infection at 4.1%, corresponding to approximately 316 million infected individuals [4]. Recent recommendations from the Centers for Disease Control and Prevention (CDC) suggest HBV screening at least once during a lifetime for adults aged ≥18 years [5].
The prevalence of metastatic disease in HCC has been reported to be 11.2-25.5%, with the lungs (55%), lymph nodes (41%) and bones (7%) being the most commonly affected sites [6]. HCC has a strong tendency for macro-vascular invasion, with a high incidence of portal and hepatic vein thrombosis (35-44% and 2-12%, respectively) [7].
Direct tumor extension from the hepatic veins into the inferior vena cava and the RA is the primary mechanism of cardiac involvement in HCC, with a reported incidence of 1.4-4.9% [8]. Jun et al. [9] analyzed a cohort of 665 patients with HCC, 33 of which had RA invasion, and identified the following risk factors for its extension: invasion of the hepatic vein, simultaneous invasion of the portal vein and the inferior vena cava, the presence of multinodular HCC and advanced disease stage (classified as modified TNM staging ≥ Iva). Tumor size and elevated alphafetoprotein levels are also associated with vascular invasion [10]. The clinical presentation of HCC with RA extension is primarily influenced by the size of the intracardiac component and can range from asymptomatic (39.5%) to bilateral lower limb edema (37.5%) and exertional dyspnea [11].
In this case, considering the presence of pulmonary metastasis and extensive liver involvement, systemic treatment emerged as the optimal option. However, due to the presence of pulmonary thromboembolism and the need for anticoagulation, as well as the presence of active hepatitis B infection, the utilization of bevacizumab-atezolizumab was precluded. Following the development of gastrointestinal intolerance to sorafenib, alternative therapies such as ramucirumab were considered. However, the deterioration in clinical functional status and liver function led to the progression to BCLC-D staging, preventing the initiation of a second-line systemic therapy. While aggressive approaches and multi-modality have been reported in clinical cases, when HCC presents with cardiac involvement, it significantly restricts therapeutic options, and there is no consensus regarding the optimal treatment. In the absence of extra-hepatic spread, transarterial chemoembolization (TACE) has been documented in earlier stages of HCC with atrial macrovascular invasion [12, 13]. Kolarich et al. [13] reported a retrospective series of 8 patients with macrovascular invasion treated with TACE, supplemented by lenvatinib in 4 cases, resulting in an 86 ± 19% reduction in intra-atrial tumor burden. Although surgery has shown good technical success, even in cases with extra-hepatic metastasis in patients with good hepatic reserve, with a 1-year survival of 29.2% in those undergoing non-curative surgery [14], the multicentric nature of the tumor burden precluded surgical intervention in our case. Wakayama et al. [14] described a retrospective cohort of 5 patients who underwent curative resection, all of whom experienced postoperative recurrence, with a median recurrence-free survival of 3.8 months. More recently, a case report detailed a HCC with RA involvement managed with multimodal therapy, incorporating systemic therapy followed by TACE and liver resection [15]. Despite the documentation of more aggressive and multimodality treatments in the literature, evidence regarding their efficacy and impact on survival remains sparse.
The prognosis for HCC with intra-cardiac involvement remains poor, with a median survival range of 1-4 months [15]. Cardiopulmonary complications include pulmonary embolism, heart failure, life-threatening arrhythmias, and systemic metastasis, with heart failure and sudden cardiac death being the primary causes of mortality, affecting up to 25% of patients [15].
The severity and complexity of the case, combined with the patient’s young age, make this an ethically challenging situation. The multidisciplinary interaction with oncology and palliative care was extremely important, not only for therapeutic decisions but also to ensure a dignified end of life.
This case report presents a rare case of HCC with extensive vascular and cardiac involvement in a young patient with previously unknown non-cirrhotic HBV infection. The presentation with mainly cardiac symptoms and the investigation of a cardiac mass that led to the diagnosis makes this case unusual and interesting. Furthermore, it highlights the importance of HBV screening and diagnosis since it may lead to timely detection of HCC - a crucial step in averting diagnosis at advanced stages.
We acknowledge the limitations of a case report approach such as the lack of ability to generalize or to infer a cause-effect association. Particularly in this rare pre-sentation of HCC with cardiac involvement, further research is needed to determine the optimal approach to this complex situation.

