











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Yersinia enterocolitica (YE), an anaerobic gram-negative bacillus within the Enterobacteriaceae family, is a notable cause of food-borne gastroenteritis in Europe. It primarily affects the ileocaecal region, appendix, and mesenteric lymph nodes, leading to terminal ileitis, enteritis, mesenteric lymphadenitis, pseudo-appendicitis, and septicaemia. Transmission to humans commonly occurs through the faecal-oral route via contaminated water, food, soil, and animal sources, with rodents, domestic animals, and birds as significant reservoirs. Consumption of raw pork, contaminated water, or vegetables can trigger outbreaks of YE infection [1, 2].
The clinical spectrum of YE infection often resembles inflammatory bowel disease, acute appendicitis, and even neoplasia, particularly lymphoma, posing a diagnostic challenge [3-5]. Clinical, endoscopic, and histological features of YE infection can mimic those of Crohn’s disease (CD). Furthermore, patients may present with extra-intestinal manifestations such as erythema nodosum and reactive arthritis, commonly observed in CD [6]. The endoscopic appearance of Yersiniosis usually includes aphthoid or irregular-shaped ulcers and thickened nodular mucosa in the terminal ileum and cecum, in contrast to the cobblestone pattern typically seen in CD [3]. Nevertheless, the endoscopic appearance is not always typical and the distinction between both diseases may sometimes be difficult. This clinical case describes a unique presentation of YE infection resembling an initial diagnosis of CD, with overlapping endoscopic features and isolated colonic involvement, a scenario, to our knowledge, not previously described.
Case Report
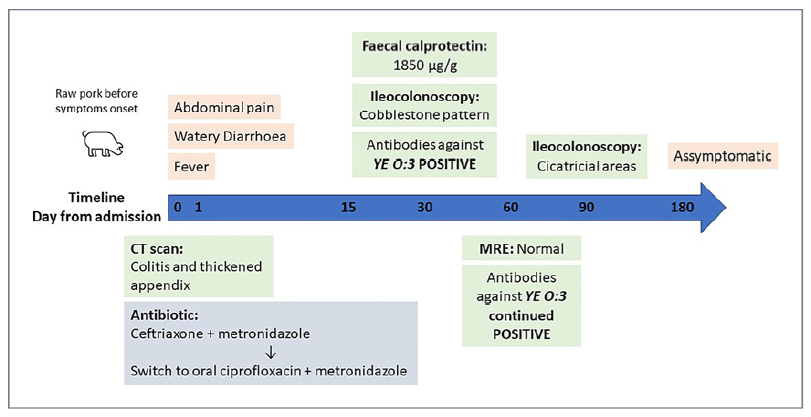
A 48-year-old female patient sought care at the Emergency Department with a 15-day history of non-bloody watery diarrhoea (7-8 bowel movements per day), including nocturnal episodes, accompanied by fever, lower abdominal pain, nausea, and vomiting. Denying any weight loss, she recalled consuming an undercooked pork steak at a restaurant before symptom onset, although none of her dining companions reported similar symptoms. A detailed timeline and clinical course of the disease are shown in Figure 1.
The patient had a significant medical history of a BRCA1 mutation with a previous diagnosis of localized breast cancer 9 years ago, for which she underwent bilateral mastectomy, radiotherapy, and hormone therapy. Subsequently, she underwent hysterectomy and bilateral oophorectomy. Additionally, she had a history of smoking and psoriasis vulgaris, with letrozole being her only medication over the past 4 years.
On examination at the Emergency Department, she was hemodynamically stable but exhibited tenderness in the right lower quadrant. Laboratory investigations revealed anaemia, elevated platelet count, and increased C-reactive protein (CRP) and procalcitonin (shown in Table 1). Given the significant right lower quadrant abdominal pain, a CT scan was performed, revealing thickening of the bowel wall in the ascending, transverse, and descending colon, with a slight thickening of the appendix, although without significant mesenteric fat hypertrophy (shown in Fig. 2). The surgical team assessed the patient and concluded that the presentation was atypical for appendicitis.
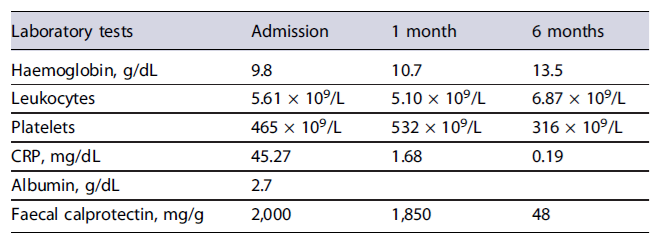
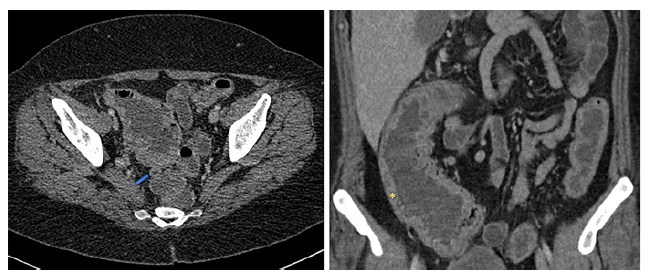
Fig. 2. CT scan at admission demonstrating a thickened appendix (left image, blue arrow) and a thickening of the bowel wall in the ascending colon (right image, yellow*).
Due to the presence of diarrhoea, abdominal pain, and fever, a diagnosis of infectious colitis was considered. Stool samples were collected for bacterial, parasitological and Clostridioides difficile infection assessment. Also, testing for Salmonella and YE infection was performed, alongside faecal calprotectin measurement and blood cultures analysis. Empirical antibiotic therapy with ceftriaxone and metronidazole was initiated, leading to significant clinical improvement within 48 h, marked by decreased frequency of bowel movements, resolution of fever, and reduction in CRP levels. Subsequently, the patient was discharged and prescribed 1 week of oral antibiotic therapy.
Despite initial improvement, the patient’s post-discharge assessment revealed the presence of severe fatigue and continuous diarrhoea with 2-3 bowel movements per day along with persistent microcytic anaemia, low iron stores, severe hypoalbuminemia (2.7 g/dL), and elevated faecal calprotectin (2,000 μg/g). Therefore, further investigation was deemed necessary. One month after the initial presentation, an endoscopic evaluation was conducted revealing normal mucosa in the terminal ileum but large, deep ulcerations in the ascending and transverse colon, with skip areas of normal mucosa resulting in a cobblestone-like appearance (shown in Fig. 3). The descending and sigmoid colon displayed smaller ulcers (less than 10 mm) with milder inflammation compared to the right colon. Histopathological examination revealed nonspecific findings with an intact ileal mucosal architecture with slight lymphoplasmacytic infiltrate in the lamina propria and a colonic mucosa with normal caliciform cell population without architectural distortion, despite a moderate inflammatory infiltrate, but without epithelial lymphocytosis, basal membrane thickening, granulomas, or cryptitis.
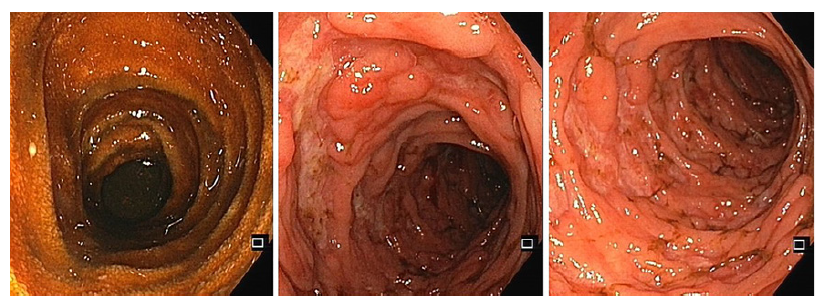
Fig. 3. Ileocolonoscopy 1 month after admission demonstrating a normal mucosa of the terminal ileum (left image) and a transverse and ascending colon with deep and large ulcers with cobblestone pattern (middle and right image).
Pending microbiological test results from the initial hospitalization were negative, including blood and stool cultures, Widal reaction for Salmonella infection, and Clostridioides difficile toxin. However, faecal calprotectin levels (1,850 μg/g) persisted elevated, while serological testing revealed positive antibodies against YE O:3.
Given the hypothesis of inaugural CD due to suggestive endoscopic findings, despite a positive YE serology, which could be a superimposed infection, a magnetic resonance enterography (MRE) was requested to assess small bowel involvement, which was only performed 2 months after the presentation. The MRE showed resolution of colonic bowel wall thickening, without complications such as stenosis or penetrating lesions.
The disparities observed among the endoscopic findings, histopathological results, and MRE evaluation did not permit a conclusive diagnosis. Consequently, a subsequent endoscopic reassessment was conducted. This follow-up evaluation revealed substantial improvement, characterized by the absence of ulcerations and restoration of the typical vascular pattern of the colonic mucosa. Additionally, evidence of scar tissue from prior ulcerations was noted (shown in Fig. 4). Histopathology demonstrated preserved architecture, accompanied by oedema, vascular congestion, and mild inflammatory infiltrate yet no evidence of granulomas. Culture and polymerase chain reaction analyses yielded negative results for Mycobacterium tuberculosis. No stool or biopsy cultures were conducted to detect YE infection since the diagnostic yield was expected to be low at this time.
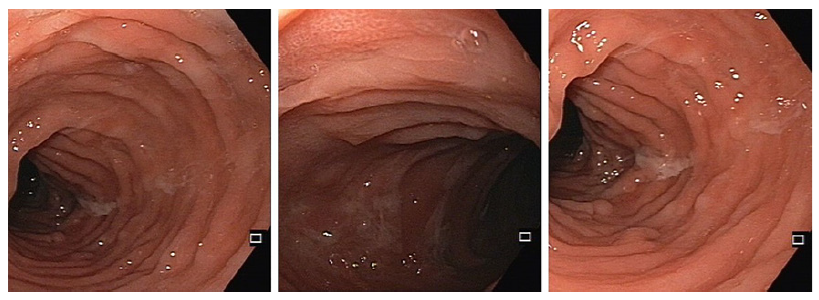
Fig. 4. Ileocolonoscopy 3 months following the initial admission demonstrating complete resolution of the endoscopic pattern with some cicatricial areas of previous deep ulcers (middle image).
Following the second colonoscopy, the patient exhibited remarkable improvement without therapeutic interventions. At 6-month follow-up, she remained asymptomatic with normalized bowel movements, resolution of anaemia (Hb 13.5 g/dL), and decreased faecal calprotectin levels (48 μg/g) (shown in Table 1). Consequently, a probable diagnosis of YE infection was made based on the clinical presentation with spontaneous improvement and epidemiological association.
Differential Diagnosis
The acute/subacute presentation initially pointed towards an infectious aetiology for the colitis. However, the presence of additional factors such as anaemia, thrombocytosis, and consistently elevated CRP in a patient with an autoimmune background and smoking history raised suspicion of a chronic condition, such as CD. Furthermore, the initial endoscopic examination revealed a cobblestone appearance, which, though nonspecific, strongly suggested CD, particularly when compared to other differential di-agnoses like tuberculosis or Behçet’sdisease [7].
Despite positive serology for YE O:3, the most reported strain in human Yersiniosis, the isolated colonic involvement was unusual, casting doubt on YE infection as the sole culprit. Nevertheless, upon retrospective analysis, considering the patient’s presentation with pseudo-appendicitis and radiological evidence primarily affecting the right colon, a diagnosis of probable Yersiniosis gained support. While the terminal ileum is typically the primary site affected by YE infection, the involvement of other segments, including the colon, remains plausible.
Discussion
The 2021 epidemiological report from the European Centre for Disease Prevention and Control (ECDC) underscored Yersiniosis as the third most frequently reported gastrointestinal infection in the European Union/European Economic Area, after campylobacteriosis and salmonellosis. Notably, 2021 witnessed an 11.8%increase in notification rates compared to 2020 and the pre-pandemic years from 2017 to 2019. Germany, closely followed by France, reported the highest number of cases, in contrast to Portugal, where only 34 cases per 100,000 inhabitants were reported in 2021 [2]. YE O:3 strains are the most frequently encountered in Europe, primarily associated with pork products. Our patient’s consumption of raw pork before symptom onset aligns with the typical incubation period of 4-10 days observed in Yersiniosis cases.
A previous review of endoscopic findings in YE infection highlighted a terminal ileum involvement, with no abnormalities in the left colon. Endoscopic findings typically featured round or oval elevations, and shallow and irregular ulcers scattered throughout an oedematous mucosa. However, this review had the limitation of including only 8 patients [8]. Despite this, a recent report showcased a cobblestone appearance resembling CD in a patient with sole terminal ileum involvement, contrasting with our case, which exhibited a similar endoscopic pattern but with exclusive colonic involvement, marking, to our knowledge, the first instance of this presentation in Yersiniosis [9]. However, the initial endoscopic assessment in our case was conducted approximately 6 weeks after the onset of the symptoms. Thus, the absence of ileal involvement at this evaluation does not exclude prior inflammation as the initial radiological findings indicated a thickening of the appendix and more pronounced radiological activity in the right colon. It is important to acknowledge the limitations in characterizing the endoscopic involvement of YE infection, as endoscopy is typically not warranted for Yersiniosis diagnosis and is reserved for cases with diagnostic uncertainty or need for biopsy specimen collection. Also, previous reviews have not established a clear correlation between endoscopic findings and infection duration. Nonetheless, earlier case reports based on imaging evaluations showed ulceration appearing 4-5 weeks after symptom onset and ileal perforation occurring 5 weeks afterwards [10, 11].
Similarly to previous reports, the endoscopic findings in our case, along with the subacute duration of the symptoms, raised suspicion of CD, supported by laboratory changes including anaemia, thrombocytosis, and hypoalbuminemia [9]. However, in patients presenting with subacute abdominal pain and evidence of enteritis or enterocolitis, it is crucial to consider other potential causes, such as drug-induced enterocolitis (especially with non-steroidal anti-inflammatory drugs or aspirin), intestinal tuberculosis, other infectious enterocolitis, collagen diseases, vascular lesions, and neoplasia like lymphoma. There is a high risk of clinical and histological mimicry between CD and YE infection as they have similar clinical manifestations, often affect the ileocaecal region, and can both present with granulomas on histopathological examination. However, YE infection may be distinguished histologically by central necrosis of the granulomas and a perigranulomatous lymphoid cuff [3].
According to the ECDC definition, our case report represents a probable diagnosis of Yersiniosis since it meets the clinical criteria including fever, diarrhoea, and abdominal pain, along with an epidemiological link of exposure to a common source of infection [12]. For a definite diagnosis of Yersiniosis, isolation of the organism in a clinical specimen is necessary, with prolonged low-temperature culture in a selective growth medium being the most sensitive method [13]. Alternatively, virulence genes can be detected using molecular techniques, though these are not always readily available. The presence of positive serology is not part of the diagnostic criteria. Nevertheless, it might be used as a screening tool for the presence of the infection, although it requires further confirmation, most commonly through stool culture.
While an infectious aetiology was initially considered, YE was not immediately suspected. Only standard stool cultures were ordered, without a specific incubation growth medium for YE. Additionally, at the time of the endoscopic assessment, a chronic inflammatory condition was suspected due to the subacute course of the diarrhoea and suggestive laboratory features. This suspicion was further reinforced by endoscopic findings compatible with CD, leading to the omission of specific cold culture biopsies for YE. It is important to highlight that the microbiologist should be aware of the suspicion of Yersininosis so that specific molecular and cultural tests can be ordered, and, if necessary, performed in another institution as it would have been relevant in our case. Although some studies have suggested an association between YE infection and CD, further research has failed to find significant differences in YE infection rates between CD patients and controls. These discrepancies may result from variations in the diagnostic methods used to detect YE and from the different symptoms of YE infection, which can vary according to the virulence of the strains. Moreover, establishing an association between these two conditions does not necessarily mean a causal link.
While most cases of YE infection are self-limiting and do not require antibiotic treatment, in certain populations, such as the elderly, immunocompromised individuals, diabetics, iron overload, alcoholism, or chronic diseases, treatment should be considered. Aminoglyco-sides and fluoroquinolones are the most used antibiotics. Trimethoprim-sulfamethoxazole combination, tetracyclines, and third-generation cephalosporins are other options [1, 4]. In conclusion, it is imperative to consider infectious aetiologies, such as Yersiniosis, when evaluating patients with acute or subacute abdominal pain and diarrhoea, and this diagnostic suspicion should be promptly communicated to the microbiologist.

