











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Gastric heterotopia (GH) is characterized by the presence of differentiated gastric mucosa tissue outside the stomach, known as inlet patch, most commonly located in the proximal esophagus [1, 2]. The incidence ranges between 0.1 and 10% in adults [2]. Most patients with GH are asymptomatic; however, symptoms such as globus sensation, dysphagia, and odynophagia are associated due to acid secretion from the gastric mucosa [2, 3]. Complications including esophageal strictures have been reported, but polyps are rarely seen [4]. Despite the generally low incidence of relevant manifestations reported in the literature, controversies remain regarding the clinical significance of this condition.
Clinical Case
A 53-year-old man was referred for management of a sessile polyp (Paris 0-Is) in the proximal esophagus, identified during an esophagogastroduodenoscopy performed due to heartburn and regurgitation. Biopsies were compatible with a hyperplastic polyp.
The patient’s medical history includes heavy tobacco consumption. Additionally, he was taking esomeprazole at a dose of 40 mg.
We repeated upper gastrointestinal endoscopy and observed two areas of pink mucosa oppositely positioned in the proximal esophagus (18 cm from the incisors), suggesting GH. One of these areas had a polypoid morphology with congestive, friable, and erosive mucosa measuring approximately 12 mm (Fig. 1). Narrow-band imaging evaluation showed a preserved glandular, vascular pattern (Fig. 2). Biopsies were taken from the lesion and anatomopathological assessment revealed fragments of gastric-type mucosa, consisting of occasional poorly oriented foveolar structures compatible with ulcerated GH. There was no metaplasia or dysplasia. No H. pylori-like microorganisms were observed in GH (Fig. 3). A multidisciplinary approach led us to decide on an expectant strategy due to its probable benign course. A follow-up endoscopy was performed, and the polypshowednosignificant changes from the prior examination.
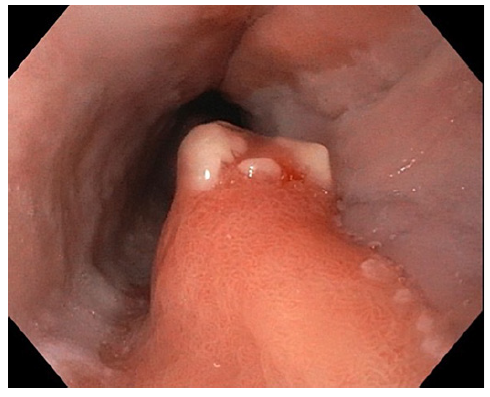
Fig. 1 Congestive and friable polyp arising from esophageal inlet patch in the proximal esophagus, in contralateral position to another inlet patch.
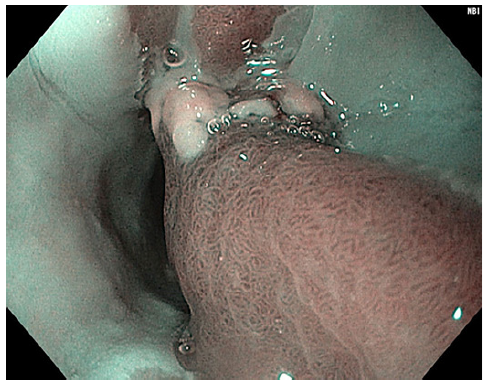
Fig. 2 Narrow-band imaging assessment of the polyp showing a preserved glandular and vascular pattern.
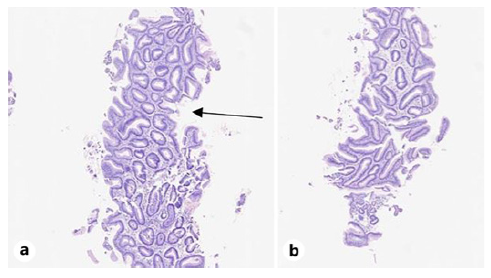
Fig. 3 Proximal esophagus: two distinct fragments (a, b) of gastric-type mucosa with foveolar structures (black arrow). Hematoxylin-eosin staining. ob2x.
A diagnosis of GH with a polypoid morphology was made, which is compatible with a hyperplastic polyp. Hyperplastic polyps rarely originate from esophageal inlet patches and their potential carcinogenic pathway has not been fully documented. To our knowledge, only a few case reports of GH with polypoid morphology exist in the literature [2, 4]. Further research is needed to determine the most appropriate management of these patients.

