











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Ascites is the most common complication of advanced chronic liver disease, with an incidence of 5-10% of patients annually in the compensated stage [1]. The main pathophysiological mechanism involved appears to be sodium retention due to overactivation of the renin-angiotensin-aldosterone system and sympathetic nervous system, which culminates in an accumulation of fluid in the extracellular space [1]. The emergence of ascites has a significant impact on quality of life (QoL), and is associated with complications such as bacterial peritonitis (BP), ventilatory dysfunction, abdominal hernias, worsening of renal function, and can result in hospitalization [1, 2]. Initial therapy includes loop diuretics and aldosterone antagonists [1]. However, as liver disease progresses to end-stage liver disease (ESLD), patients may develop refractory ascites (RAs), as this approach becomes ineffective and is hindered by complications.
At ESLD, survival ranges from 6 months to 1 year, with few validated therapies available [1]. Liver transplantation, the most effective treatment, is not feasible for the majority of patients, and many are also unsuitable candidates for transjugular intrahepatic portosystemic shunt. Furthermore, other palliative interventions, such as surgical peritoneovenous shunts, are used sparingly due to the high rate of associated complications [2, 3], while the Alfapump® system is available only in select centers and has a significant complication rate of 85% [1-3]. Consequently, most patients resort to large-volume paracentesis (LVP) as their only option, requiring regular hospital visits lasting several hours, potentially leading to complications (10-15%) such as post-paracentesis circulatory dysfunction and worsening kidney function, often necessitating albumin replacement [1, 2].
A topic in hepatology that has recently gained prominence is the necessity for palliative care for this population. Similar to other conditions, these patients experience reduced survival rates and a significant symptomatic burden, which greatly impacts their QoL [1, 2, 4]. Given these challenges, the utilization of long-term abdominal drains (LTAD) has emerged as a novel therapeutic opportunity increasingly used in RA associated with ESLD. The use of this approach in the ESLD population is associated with several concerns including the risk of infectious and worsening renal function [2-4].
Objectives
This review aims to describe the safety, effectiveness, and impact on the QoL of LTAD in ESLD-related ascites.
Methods
A systematic review of research articles on the utili-zation of LTADs for advanced chronic liver disease, published from 1 January 2001 to 1 June 2024, was conducted. The literature search and the verification of inclusion and exclusion criteria were performed by two independent reviewers (D.S., A.G.). An initial search was conducted using PubMed-MEDLINE, Embase, and Google Scholar. Medical subject headings (MeSH) applied were the following: (cirrhosis OR chronic liver disease) AND refractory ascites AND (permanent-tunneled peritoneal catheter OR tunneled catheter OR indwelling catheter OR long-term abdominal drains). The methodology followed Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) recommendations (see online supplementary material at https://doi.org/10.1159/000543713). Screening and testing for eligibility were performed based on English-written abstracts. A grid was constructed to assess articles for eligibility and select them for inclusion, according to specific inclusion and exclusion criteria.
Inclusion Criteria
English full-text articles from peer-reviewed journals, including online publications ahead of print, within the specified time frame.
Retrospective and prospective studies, including cohort, case series, case-control, randomized controlled trials and case reports.
Studies involving adults.
Studies on the safety, effectiveness, and benefits of LTADs in chronic liver disease-associated RAs. Exclusion Criteria
Review articles (systematic and non-systematic), comments, letters, and book chapters.
Conference abstracts, oral communications, and posters.
Papers focused on children or adolescents or authored by pediatric institutions.
Studies on LTADs used only for ascites unrelated to chronic liver disease or those that did not separately report data for chronic liver disease-related ascites.
The full text of selected relevant studies was then evaluated by two researchers (D.S. and A.G.) independently, according to the inclusion criteria described above. Other authors (P.G. and I.C.) intervened in case of disagreement. The quality of the studies was assessed using the Newcastle-Ottawa Scale (NOS), which awarded stars based on factors such as participant selection, comparability of study groups, and outcome measurement.
In this systematic review, the outcomes used to evaluate LTAD were categorized into three domains: effectiveness, safety, and QoL. Effectiveness was assessed by measuring technical success in LTAD implantation and the need for additional LVP while the device remained in situ. Safety outcomes focused on both infectious and noninfectious complications and mortality rates. Finally, QoL was assessed using both subjective and objective methods.
Results
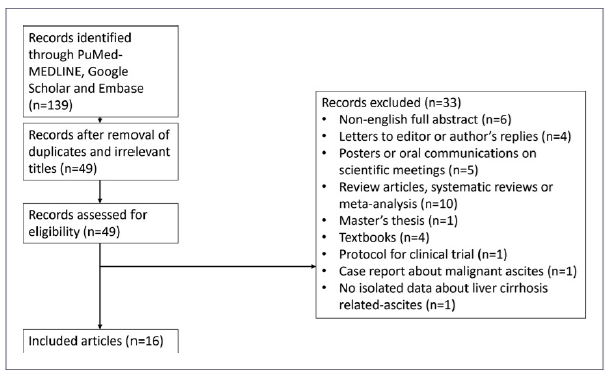
One hundred thirty-nine references were initially identified in PubMed-MEDLINE, Embase, and Google Scholar. After the irrelevant titles were removed, 49 records underwent screening, resulting in 16 eligible articles and 33 exclusions. The study selection process is shown in Figure 1.
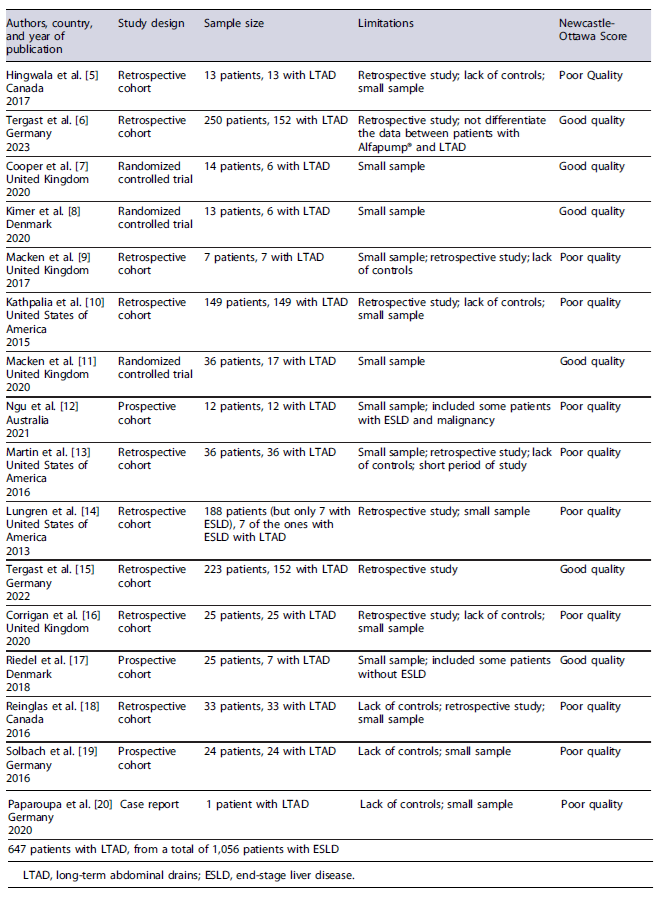
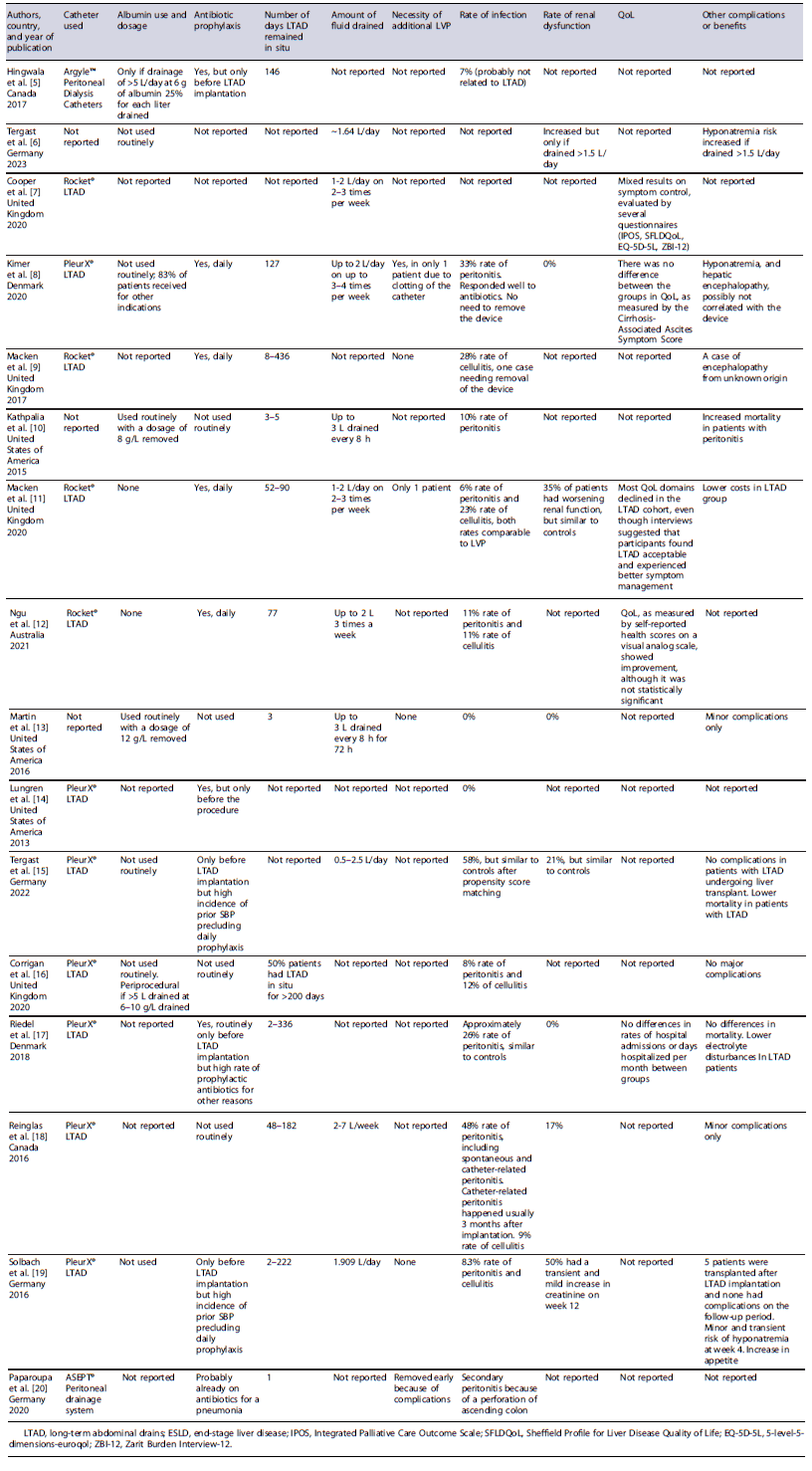
NOS quality assessment and limitations for all the 16 articles selected for review are summarized in Table 1. The main characteristics of the articles selected for review are summarized in Table 2.
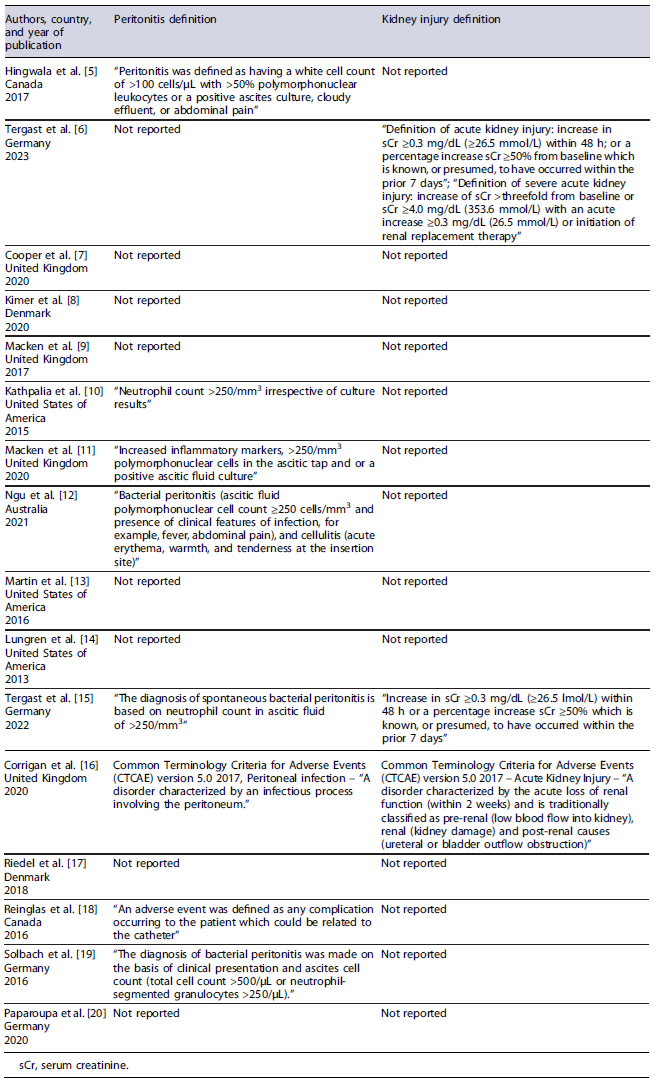
The included studies presented heterogeneity in design, reported on different types of LTAD, and were generally of low quality, with many having limited statistical power due to small sample sizes. Infection and kidney injury were defined more heterogeneously across the studies. To clarify these definitions, we have summarized them in Table 3.
A total of 1,056 patients with ESLD were analyzed, 647 of whom received LTAD. The reported age range across studies spanned from 44 to 83 years. Male patients comprised between 43% and 79% of the sample, while females ranged from 21% to 57%. The underlying etiologies also varied widely. Alcohol-related causes were the most frequent, representing 29-81% of cases. Other common causes included metabolic-associated steatotic liver disease, affecting 16%-41% of patients, and viral hepatitis, which accounted for up to 39% in certain studies. Less common etiologies included cryptogenic causes, autoimmune liver diseases, and other metabolic or cardiac conditions.
Liver disease severity was assessed using the Model for End-Stage Liver Disease (MELD) score in 13 of the 16 studies, with scores ranging from 5 to 31. The Child-Pugh score was employed in 9 studies; among these, 4 reported scores ranging from 5 to 11, while the remaining 4 studies categorized patients by stage, resulting in 61 patients classified as Child-Pugh B and 48 as Child-Pugh C.
Patients were managed in various settings, including at home (n = 440) and in hospitals (n = 185), with some studies not specifying the primary drainage location. Ascites drainage was performed by patients, caregivers, or nurses, though most studies did not specify who con-ducted the procedure.
Effectiveness
Both non-tunneled and tunneled catheters, with either one or two cuffs, were utilized. LTAD implantation was typically performed by interventional radiologists or hepatologists under ultrasound guidance and occasionally supplemented by fluoroscopy.
Technical success in LTAD implantation was 100% in all analyzed studies, regardless of the catheter type, with PleurX® and Rocket® being the most commonly reported. Although not all studies evaluated effectiveness - defined as the absence of the need for additional drainage via LVP while the LTAD remained in situ - those that did, reported that additional drainage was rarely necessary. When additional drainage was required, it was typically due to transient catheter blockage or dislodgment. In the cohort of 647 patients with LTAD, catheter placement durations ranged from 1 to 436 days.
Safety
Safety was assessed based on complications associated with the device, which can be either infectious or noninfectious, as well as mortality following drain implantation. Infectious complications include primary BP, cellulitis, and secondary BP, while noninfectious complications encompass renal injury, hyponatremia, leakage, blockage, displacement, and hemorrhage.
Infectious complications were reported with an incidence ranging from 7 to 58%, with the primary complications being BP and cellulitis at the insertion site. Notably, some authors reported similar rates in control groups [11, 15, 17]. There is no consensus regarding the use of prophylactic antibiotics during LTAD implantation or on the optimal duration of therapy (periprocedural versus throughout the duration of catheter placement). The antibiotics used across studies included quinolones, cotrimoxazole, and cephalosporins. Reinglas et al. [18] reported a higher risk of infection in an uncontrolled study where catheters remained in place for more than 3 months. However, none of the studies were controlled or had follow-up periods longer than 3 months, making it difficult to compare this increased risk to standard care practices. The infection rates varied based on antibiotic use: from 0 to 48% without prophylaxis, 0-58% with periprocedural antibiotics, and 6-33% with maintenance antibiotic therapy. Most infections were managed conservatively with antibiotics, and in some cases, catheter removal was necessary. Secondary BP was also identified as a potential risk by Paparoupa et al. [20].
Concerning noninfectious complications, kidney injury incidence ranged from 17% to 50%. This wide range may be due to the large discrepancy in the volume of fluid drained between studies and the use (or absence) of albumin replacement. Albumin administration was inconsistently reported, and in most studies, it was not routinely used. Only two studies, Kathpalia et al. [10] and Martin et al. [13], routinely administered albumin, with dosages of 8 g and 12 g per liter removed, respectively. Controlled studies also demonstrated a relatively high incidence of kidney injury in control groups. Tergaist et al. [6] highlighted the relationship between fluid drainage volume and kidney injury, estimating a threshold of 1.5 L/day above which the risk of complication significantly increases. Below this threshold, even without albumin replacement, the risk of kidney injury appears to be similar to standard of care, where albumin is routinely administered. Hyponatremia was another noted risk, which, according to Tergaist et al.[6], only becomes apparent after exceeding the 1.5 L/day drainage threshold.
Most studies also reported minor complications such as leakage, blockage, and displacement, which were generally self-limited or resolved conservatively. For instance, was typically resolved with an additional suture at the catheter insertion site, while blockage or displacement was addressed through catheter replacement. The incidence of leakage, obstruction, and displacement ranged from 12 to 29%, 4-17, 6%, and 6-10%, respectively, across the studies. No bleeding complications were reported.
Some authors [15, 19] have noted successful LTAD placement in patients who later underwent liver transplantation, even in cases involving infections related to the device, without significant complications. This sug-gests that LTAD could potentially be used as a bridge to transplantation in the future, supported by reports involving a total of 10 patients.
Few studies assessed the impact of LTAD on mortality. Riedel et al. [17] reported no impact on mortality. Kathpalia et al. [10] reported a higher mortality rate in patients with BP associated with LTAD. However, it is important to note that no antibiotic prophylaxis was administered during the procedure and that the type of catheter utilized was unspecified. Conversely, Tergast et al. [15] reported a lower mortality (hazard ratio of 0.57 on 90-day mortality) in their cohort of patients with LTAD.
Quality of Life
Few studies assessed QoL using self-reported questionnaires and interviews, with inconsistent results across studies. QoL was measured using scales such as the EuroQol 5-dimensions (EQ-5D), Chronic Liver Disease Questionnaire (CLDQ), Integrated Palliative Care Outcome Scale (IPOS), Sheffield Profile for Liver Disease Quality of Life (SFLDQoL), EuroQol-5-level-5-dimensions (EQ-5D-5L), Cirrhosis-Associated ascites Symptom (CAS) score, and Zarit Burden Interview-12 (ZBI-12). Macken et al. [11] and Cooper et al. [7] also conducted interviews with patients and nurses for qualitative data. Riedel et al. [17] extrapolated QoL from monthly hospital admissions and days hospitalized.
Kimer et al. [8] reported that the median CAS score indicated relatively poor health-related QoL at baseline. There was no significant difference between groups throughout the trial.
Riedel et al. [17] reported that for patients with ESLD, the median number of admissions was similar between the LTAD and control groups (0.6 vs. 0.8; p = 0.40). The median length of hospitalization was 5.2 days, with no significant difference between LTAD (3.1 days) and LVP (6.6 days; p = 0.14).
In Cooper et al. [7], the LTAD group showed mixed outcomes. Physical symptom scores ranged from 1 to 18, with most patients showing stabilization or slight improvement by the final visit. Emotional symptoms scored between 0 and 11, following a similar trend. Communication and practical issues scores started between 0 and 7, with slight improvements or stable results over time. ZBI-12 scores indicated reduced caregiver burden, dropping from 39 to 30. EQ-5D-5L scores varied, with some patients improving (e.g., 0.31-0.34), while others declined (e.g., 0.92 to 0.68). VAS scores also showed variability, with some improving significantly (e.g., 40-90) and others declining (e.g., 70 to 50). SFLDQoL scores showed fluctuation in symptoms, effect, and memory domains, with improvements (e.g., symptoms 63-87) and declines (e.g., effect 63 to 33). Distress and loneliness scores generally stabilized or improved, while sleep, hopelessness, and stigma scores showed varied trends. Ngu et al. [12] reported a rise in the median self-reported health score on a visual analog scale, from 50 (IQR: 30-70) to 78 (IQR: 50-85), though the change was not statistically significant (p = 0.39).
In contrast, Macken et al. [11] documented a decrease in QoL in the LTAD group compared to improvements in the LVP group. By week 12, the EQ-5D-5L score in the LTAD group slightly declined to 0.59, while the LVP group increased to 0.57, with a mean difference of 0.02. ZBI-12 scores showed a minor rise in caregiver burden for the LTAD group (17.9-18.0), while the LVP group saw a more substantial increase (14.6-20.0). IPOS-physical scores increased in the LTAD group (10.6-14.0), while decreasing in the LVP group (15.6-12.2). The LTAD group showed a slight decrease in IPOS-emotional scores (6.5), compared to a larger reduction in the LVP group (4.5). Both groups started with a mean IPOS-communication score of 2.4, but by week 12, the LTAD group remained at 2.4, while the LVP group improved to 1.8.
Discussion
LTADs have the potential to transform patient care by enabling home-based ascites drainage. Despite their extensive use in malignancy ascites with significant benefits in symptom burden and QoL, LTADs are not formally recommended for use in ESLD by most hepatology guidelines. However, some centers have begun implementing LTAD for this purpose. In 2022, a consensus document on LTAD insertion, supported by British Association for the Study of the Liver and the British Society of Gastroenterology, was published [4]. Concerns about infectious and non-infectious complications remain the primary barriers to wider LTAD use in ESLD.
Technical success rate appears to be very high across all the studies [5-20], with more recent research reporting that catheters can remain in situ for over a year [9]. Although most of the studies reported shorter catheter duration, it is essential to consider that these patients predictably have a life expectancy of only 6 months following a diagnosis of RA. This approach is generally offered to patients who are not candidates for more effective approaches like liver transplant or transjugular intrahepatic portosystemic shunt. Notably, both Tergaist et al. [15] and Solbach et al. [19] reported no complications in liver transplant patients with LTAD, suggesting its potential as a bridge to transplantation.
Drainage success with LTAD appears promising, as it can reduce diuretic dosage, with additional LVP rarely required. This probably stems from the fact that complications such as blockage or displacement, which could impede drainage, are easily resolved. Thus, LTAD demonstrate effectiveness in facilitating ascites drainage.
The variety of LTAD types, differing implantation protocols and inconsistent use of prophylactic antibiotics contribute to significant variability in outcomes. Furthermore, the amount and frequency of liquid drainage can differ widely and protocols for albumin replacement remain a topic of debate. These factors explain the wide range of complications, including kidney injury and infection rates across studies.
Significant improvements have been made in LTAD devices and their management. Initially, non-tunneled abdominal drains were used, posing a significantly higher risk of infection [2]. The tunnel creates a wider path between the peritoneal cavity and the skin, within the subcutaneous tissue. Subsequent innovations included the incorporation of cuffs providing additional protection against infection, by promoting granulation tissue growth outside the cuff sealing the tract. Unlike peritoneal dialysis, catheters which have one cuff just outside the peritoneal cavity and the other in the subcutaneous tissue, LTAD usually have only one cuff in the subcutaneous tissue. They also incorporate safety valves to prevent air and fluid from entering and to minimize fluid leakage. These mechanisms prevent infection by hampering the translocation of bacteria from the skin to the peritoneum. Antibiotic prophylaxis was not routinely administered across studies and there is ongoing debate regarding whether it should be solely periprocedurally or continued for maintenance. Standardizing clinical practice, particularly regarding the use of antibiotics, is essential for improving patient outcomes. Infection risk is a major concern in this population due to their known dysfunctions in the neutrophilic and reticuloendothelial systems, as well as low levels of immunoglobulins in ascitic fluid [18]. The primary infections of concern are risk of infection [2]. The tunnel creates a wider path between the peritoneal cavity and the skin, within the subcutaneous tissue. Subsequent innovations included the incorporation of cuffs providing additional protection against infection, by promoting granulation tissue growth outside the cuff sealing the tract. Unlike peritoneal dialysis, catheters which have one cuff just outside the peritoneal cavity and the other in the subcutaneous tissue, LTAD usually have only one cuff in the subcutaneous tissue. They also incorporate safety valves to prevent air and fluid from entering and to minimize fluid leakage. These mechanisms prevent infection by hampering the translocation of bacteria from the skin to the peritoneum. Antibiotic prophylaxis was not routinely administered across studies and there is ongoing debate regarding whether it should be solely periprocedurally or continued for maintenance. Standardizing clinical practice, particularly regarding the use of antibiotics, is essential for improving patient outcomes. Infection risk is a major concern in this population due to their known dysfunctions in the neutrophilic and reticuloendothelial systems, as well as low levels of immunoglobulins in ascitic fluid [18]. The primary infections of concern are may occur, where the microorganisms originate from the skin rather than the enteric microbiome.
Therefore, to accurately diagnose BP in LTAD patients, it is advisable to perform a diagnostic tap for cell count and culture from both peritoneum and the LTAD, as recommended in the consensus document published [4]. Once BP is diagnosed, it is essential to differentiate between LTAD-associated BP and spontaneous BP. This distinction is crucial, as device explantation and targeted antibiotic therapy against gram-positive microorganisms may be beneficial for the former group. However, most of the analyzed studies do not differentiate between these two subtypes, hampering strong conclusions about the risk of device-related BP in patients with LTAD.
Since granulation tissue growth around the cuffs takes time to develop, the tract is not sealed at the time of the implantation. Therefore, periprocedural antibiotic prophylaxis seems rational despite one study that did not employ it reported acceptable infection rates [16]. Furthermore, as LTAD can potentially lead to BP it is advisable to exclude BP before implantation [4].
It is important to note that most reported infections are easily resolved with antibiotics or through device explantation. Once the infection is addressed, the device can often be safely reimplanted [9].
Kidney injury is a major concern for ESLD patients due to their constant state of relative hypovolemia [1], making them more susceptible to worsening kidney function in the presence of precipitating factors. Additionally, kidney injury worsens the prognosis [1] of these patients, highlighting the importance of preserving kidney function. It is hypothesized that grade III ascites can reduce renal venous flow due to increased intra-abdominal pressure. Furthermore, LVP performed without albumin replacement is associated with deteriorating kidney function, likely due to the rapid drainage of large volumes of fluid over a short period - sometimes exceeding 10 L within a few hours - aggravating the relative hypovolemia state. Therefore, it stands to reason that draining smaller amounts of fluid more frequently may be a safer approach.
Although few of the analyzed studies focused on this subject, LTAD appear to be safe when smaller volumes - particularly <1.5 L/day - are drained 2-3 times a week, even without albumin replacement [6]. In controlled studies [11, 15], kidney injury incidence seems comparable between patients submitted to LVP and LTAD, despite only the LVP group receiving routine albumin replacement. No study has conclusively reported an increased risk of hyponatremia, hepatic encephalopathy, or kidney injury when adhering to these limits and no post-paracentesis circulatory dysfunction have been observed within this range. However, caution is warranted in interpreting these findings, as some LTAD patients have reduced their diuretic dosage while using the devices, whereas some LVP patients have not, which could bias interpretation [19]. Nonetheless, the fact that LTAD patients could reduce their diuretic dosage and did not require additional LVP seems to confer additional protection against kidney injury, given the association between diuretic use and kidney complications. Other complications include leakage (usually self-limiting but can be addressed with an extra suture if it persists), LTAD blockage, or displacement which may necessitate replacement.
Bleeding is another potential complication associated with LTAD, particularly concerning in the ESLD population due to compromised hemostasis [1, 4]. It often originates from the abdominal wall vessels, such as the superior and inferior epigastric arteries, as well as portosystemic collateral vessels. To mitigate this risk, the peritoneal wall is usually accessed, away from the epigastric arteries, which are generally located 4 cm lateral to the umbilical scar. Ultrasound guidance, particularly Doppler, is utilized to ensure avoid vessels in the chosen tract. It is also advisable to check platelet count and coagulation parameters and to discontinue anticoagulants and antiplatelet medications prior LTAD implantation [4]. Despite being a high-risk procedure in a vulnerable population, bleeding rates reported with LTAD implantation are typically low and often self-limiting [4], as our analysis showed.
Rare but severe complications include bowel perforation and death; however, the latter may be attributed to other causes in this specific case [20]. The most recent evidence suggests that LTAD do not negatively affect mortality, likely due to improved periprocedural management [15, 17]. Additionally, several cases documented LTAD use for extended periods [9] supporting the notion of its safety, especially when considering the limited life expectancy of this population.
Paradoxically, it has been reported that Child-Pugh classification and MELD scores, do not correlate with the rate of infection. Thus, LTAD appear to be safe even in patients with advanced disease [18].
Unfortunately, limited studies have focused on assessing the QoL in this population, despite this being a primary objective for the use of these devices. While conducting valid studies in palliative care is challenging, it is essential to implement randomized controlled trials using appropriate scales to assess symptom control in both patients and their families. Only the CAS score is specifically designed to assess the impact of ascites on QoL, but none of the self-reported questionnaires have been validated in this setting.
Data from analyzed studies are contradictory, with most reporting an overall neutral effect [8, 12, 17] or mixed results on QoL [7]. Additionally, Macken et al. [11] found that most QoL domains declined in the LTAD cohort, despite interviews indicating that participants found LTAD acceptable and experienced improved symptom management. As noted by Macken et al. [11], LTAD studies on malignant ascites similarly show inconsistent QoL improvements in questionnaire-based assessments, despite supportive evidence from qualitative data. These inconsistent results may be attributed to the lack of a validated QoL questionnaire specific to ascites and the chronic, incurable nature of RAs. With proper instruction from healthcare professionals, patients can effectively manage LTAD independently or with the assistance of a caregiver, facilitating more convenient and autonomous ascites drainage. As highlighted Macken et al. [4], the presence of caregivers and supportive social conditions are fundamental to successful device management. Moreover, LTAD may alleviate symptoms by preventing the development of tense ascites, as observed in the LVP approach.
Conclusion
LTAD are an alternative for palliative care in ESLD. Further research is needed to clarify their role as a bridge to transplantation. Caution is advised, as many supporting studies have small sample sizes and are of poor quality, leaving key questions unanswered. Nonetheless, technical advances in catheter design and procedural management have been significant. The ongoing RE-DUCe2 trial in the United Kingdom is expected to provide important insights into LTAD safety and effectiveness. More research is required, particularly on the impact of LTAD on QoL in ESLD patients, an area that remains underexplored. This review underscores the importance of palliative care in ESLD, highlighting LTAD as a potentially valuable option for RA and urging hepatologists to consider them in palliative strategies.

