











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Melanoma is a neoplasm originating from melanocytes, with cutaneous location being the most prevalent [1]. Primary mucosal melanomas arise from melanocytes located in the mucous membranes lining the respiratory, gastrointestinal, and urogenital tracts [2]. Primary gastrointestinal mucosal melanoma can occur anywhere in the gastrointestinal mucosa but is more common in the anorectal region (31.4% in the anal canal and 22.2% in the rectum), followed by the oropharyngeal area (32.8%). The esophagus (5.9%), stomach (2.7%), small intestine (2.3%), gallbladder (1.4%), and large intestine (0.9%) constitute extremely rare locations for primary melanoma [2].
Malignant melanoma of the esophagus is an uncommon cause of dysphagia and accounts for only 0.1-0.2%of esophageal neoplasms [3]. Most cases are located in the upper and middle thirds, consistent with the distribution of melanocytes in the esophageal mucosa [2]. It is more common in men (2:1), with an average age at diagnosis of 60 years [4]. The most frequent symptom is dysphagia, though weight loss and retrosternal pain are often associated [2, 4]. Diagnosis is based on esophagogastroduodenoscopy (EGD) with biopsies and immunohistochemical analysis, the latter being crucial in the amelanocytic variant [4]. Gastrointestinal melanomas are more invasive and comprise poorer prognosis than cutaneous melanomas, with overall survival of less than 5% at 5 years [2, 4, 5]. We report the case of a 70-year-old woman who experienced dysphagia, retrosternal pain, and weight loss, ultimately diagnosed with primary amelanotic malignant melanoma of the esophagus.
Case Report
A 70-year-old woman with a medical history of epilepsy, arterial hypertension, and depressive disorder was admitted to the emergency department due to a clinical condition that had been evolving for 2 months. Initially, she experienced dysphagia with solids (dysphagia score 2)[6], which progressed to dysphagia with solids and liquids (dysphagia score 4) [6] in the previous 2 days. This was accompanied by retrosternal pain, a 50% loss of body weight, and painful cervical adenopathies. She also had a slight anterior cervical swelling, related to a previous diagnosis of non-toxic multinodular goiter. There was no history of alcohol abuse or smoking. Empirical antibiotic therapy was prescribed by a primary care physician, but there was no clinical improvement. Blood tests showed a normocytic normochromic anemia with hemoglobin of 10.6 g/dL (normal range 11.8-15.8 g/dL), mean corpuscular volume of 91.6 fL (normal range 80-101 fL), and mean corpuscular hemoglobin of 31.9 pg (normal range 27-34 pg), along with a C-reactive protein level of 5.4 mg/dL (normal range <0.50 mg/dL). The EGD revealed an esophageal lesion with luminal protrusion, occupying about half of the luminal circumference, extending from 30 cm from the dental arch to the esophagogastric junction and cardia. There were extensive ulceration and friability of the mucosa at the cardia level, and multiple biopsies were performed (shown in Fig. 1). The cervical-thoracic-abdominopelvic computed tomography scan showed a solid and heterogeneous expansive lesion in the distal third of the esophagus, starting at the level of D8-D9 and extending caudally for approximately 14 cm, reaching the cranial portion of the gastric fundus that contact with the thoracic aorta and posterior cardiac chambers, and a voluminous adenopathy in the region of the celiac trunk (shown in Fig. 2). The positron emission tomography scan with 18-fluorodeoxyglucose showed the previously described lesion with a high metabolic activity, as well as adenopathies along the lesser curvature of the stomach, forming a conglomerate of 40 × 30 mm (shown in Fig. 3). Initial endoscopic biopsies were inconclusive, leading to repeated EGD with multiple biopsies directed at the most suspicious areas. The histopathological analysis with immunohistochemical staining revealed neoplastic cells with marked nuclear positivity for SOX10 and cytoplasmic positivity for vimentin, Melan-A, and HMB45, with the absence of melanin pigment (shown in Fig. 4). Dermatology evaluation was requested to exclude cutaneous, ocular, vaginal, or anal melanomas. The final diagnosis was determined to be a primary esophagocardiac malignant melanoma, amelanotic variant, grade 2, stage IV, according to the TNM classification [7]. In a multidisciplinary team meeting, the neoplasm was deemed unresectable, and the proposal was for esophageal stent placement and palliative hormone therapy. Unfortunately, the patient died 20 days after the diag-nosis, before initiating chemotherapy.
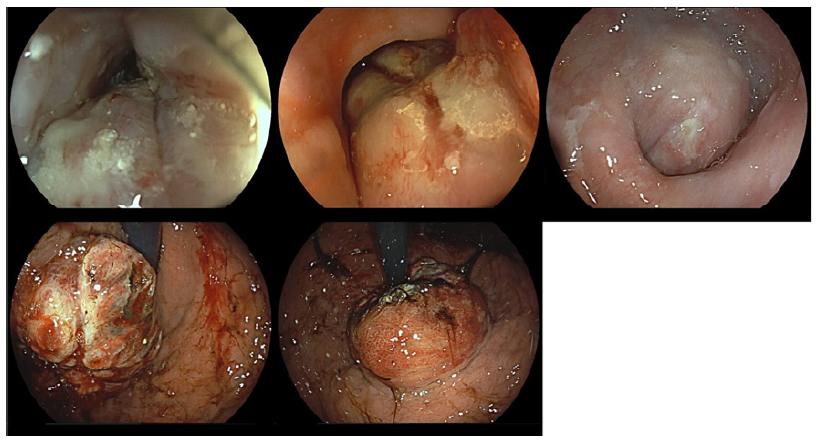
Fig. 1 EGD reveals the presence of an extensive and eccentric lesion starting at 30 cm from the dental arch, occupying approximately half of the luminal circumference at the level of the distal esophagus. There is circumferential involvement of the esophagogastric junction and the cardia, with infiltration of the mucosa and extensive ulceration and friability.
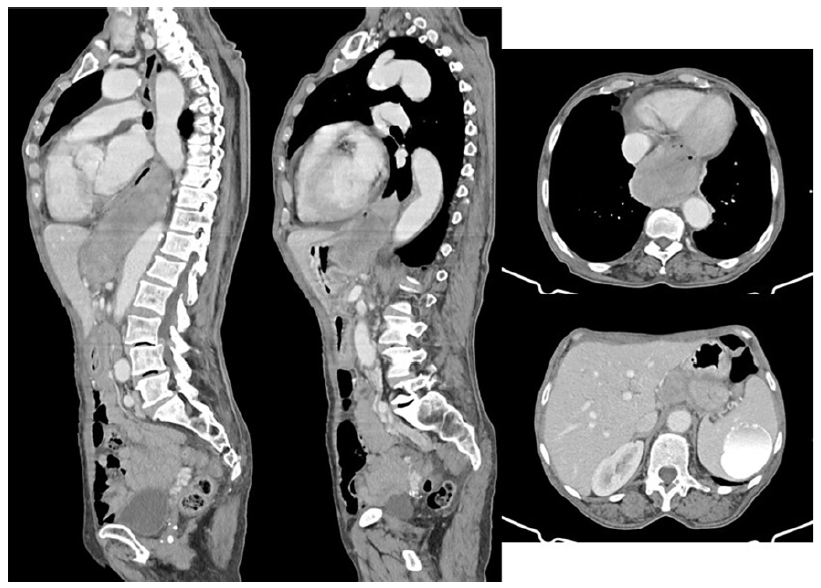
Fig. 2 Cervical-thoracic-abdominopelvic computed tomography scan showing a solid and heterogeneous expansive lesion, starting at the level of D8-D9 and extending caudally for approximately 14 cm, reaching the cranial portion of the gastric fundus with contact with the thoracic aorta and posterior cardiac chambers. Additionally, a voluminous adenopathy is observed in the region of the celiac trunk.
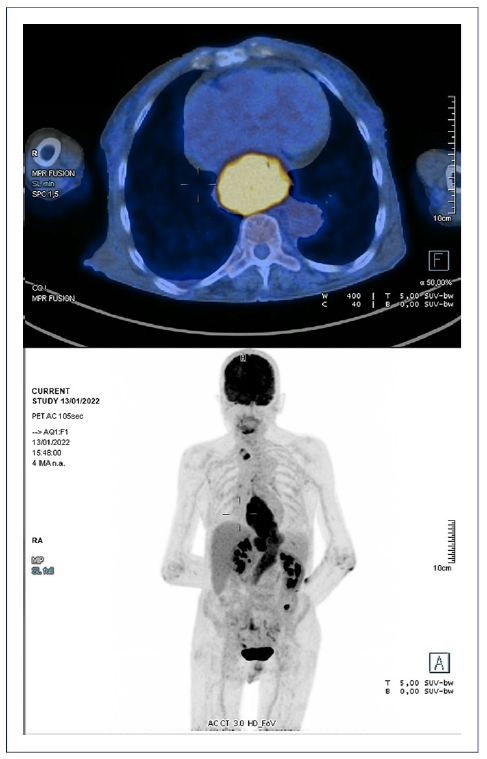
Fig. 3 18-Fluorodeoxyglucose positron emission tomography revealing an esophagogastric lesion with high metabolic activity, as well as adenopathies along the lesser curvature of the stomach, forming a conglomerate of 40 × 30 mm.
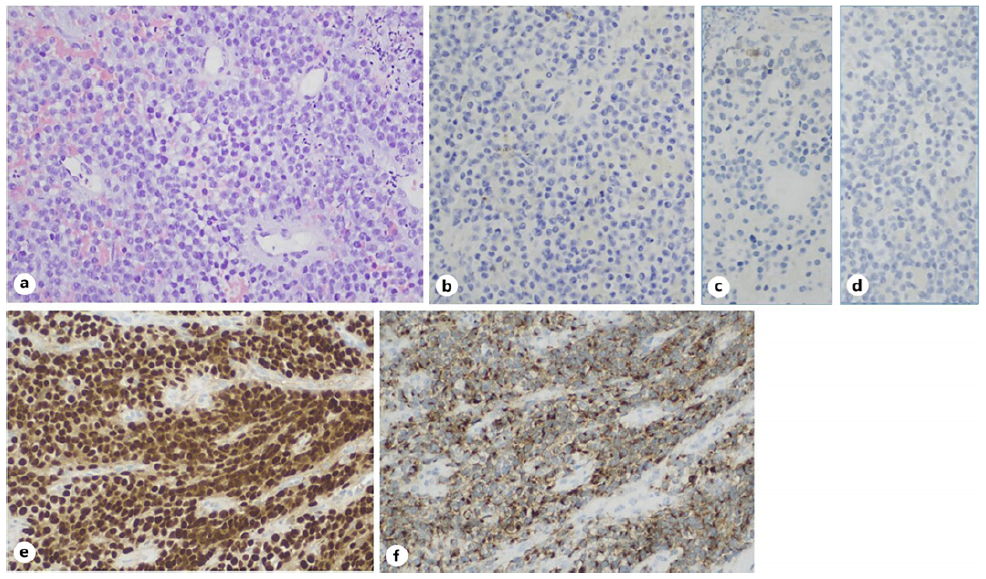
Fig. 4 Anatomopathological evaluation. a H&E 200×, a neoplasm composed of epithelioid cells with scattered apoptotic bodies, is seen. b No immunostaining for AE1/AE3 was seen. c CD20 was negative. d CD3 was also negative. e Diffuse nuclear positivity for SOX10 is seen. f Diffuse cytoplasmatic positivity for Melan-A.
Discussion
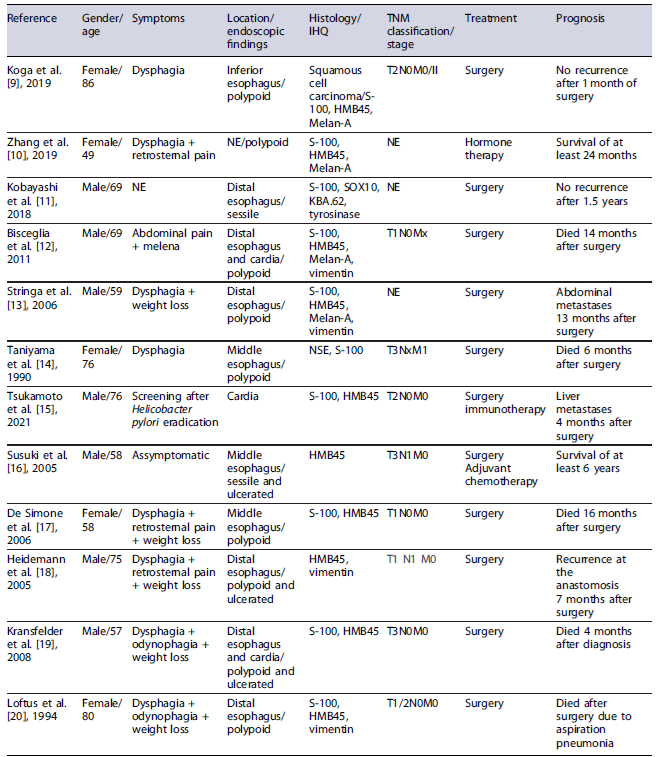
Primary malignant melanoma of the esophagus is infrequent, with only 300 cases described in the literature, and a slightly higher incidence in males [4]. It represents 0.1-0.2% of esophageal neoplasms, of which 10-25% are amelanocytic, comprising less than 0.05% of all melanoma subtypes [3, 5]. The pathogenesis for developing a primary esophageal melanoma remains poorly understood and there are no significant risk factors for this malignant condition. Table 1 describes the published cases regarding esophageal amelanocytic melanoma. The presentation is similar to other histological types of esophageal neoplasms, manifesting as dysphagia. Diagnosis requires a high degree of suspicion, based on endoscopic findings and directed histological and immunohistochemical analysis [8].
EGD can be highly suspicious in the melanocytic subtype, presenting as a dark, purple, or reddish luminal esophageal bulge, depending on the amount of melanin. However, in the amelanocytic subtype, the mucosa may appear normal in color, as in the presented case, making it challenging to differentially diagnose from other primary esophageal lesions such as squamous cell carcinoma or adenocarcinoma, as well as extrinsic lesions with esophagogastric compression and/or infiltration [5].
Additionally, secondary involvement of the lower esophageal sphincter should be part of the differential diagnosis, more commonly due to direct invasion, as in the case of primary neoplasms of the distal esophagus and proximal stomach, or metastasis, such as lung neoplasia, malignant mesothelioma, breast neoplasia, among others. Other benign conditions, such as post-surgery complications, leiomyoma, amyloidosis, neurofibromatosis, systemic sclerosis, and Chagas disease, should also be considered [21].
The histological examination with immunohisto-chemical staining of the amelanocytic subtype of melanoma reveals epithelioid neoplastic cells with indistinct borders, with moderate pleomorphism, central nucleoli, and eosinophilic cytoplasm, lacking melanin pigment but showing immunohistochemical positivity for specific melanoma markers such as S-100 (the most sensitive marker, sensitivity of 97-100%, specificity of 75-87%), HMB45 (sensitivity of 69-93%), and Melan-A (sensitivity of 97-100%, specificity of 95-100%, the most specific marker) [9, 11].
The primary malignant melanoma of the esophagus usually presents in advanced stages, with lymph node invasion detected at the time of diagnosis in 40-80% of cases. The prognosis is generally poor compared to cutaneous melanoma, with overall survival rates of less than 5% at 5 years [5, 22].
The treatment depends on the staging and functional status of the patient at the time of diagnosis. Whenever possible, definitive treatment is surgical; however, the best therapeutic strategy is still to be established given the rarity of this clinical condition [23]. In this case, the patient did not have an indication for surgical treatment and was, therefore, proposed for palliative care.
In conclusion, we report a rare case of dysphagia related to primary amelanocytic malignant melanoma of the distal esophagus and cardia, stage IV. This case emphasizes the rarity of this histological type, the importance of directing biopsies to the most suspicious areas of the lesion to increase diagnostic yield, the need for a high clinical suspicion due to its rare etiology, and the atypical endoscopic presentation caused by the amelanocytic subtype. A multidisciplinary approach is essential to determine the best therapeutic strategy.

