











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Pancreatic cysts are widely prevalent and commonly encountered in clinical practice. While prevalence according to imaging studies ranges between 2 and 15%, some autopsy data suggest a prevalence as high as 50% in aging populations [1, 2]. Even though the majority of pancreatic cystic lesions are intraductal papillary mucinous neoplasms (IPMNs) [3], with potential for malignant transformation, prospective follow-up data in a population-based setting suggest that most pancreatic cysts are harmless incidental findings [4].
IPMNs are intraductal epithelial neoplasms with potential for malignant transformation composed of mucin-producing columnar cells and may involve the main pancreatic duct (MPD) (MD-IPMN), the branch ducts (BD-IPMN), or both (mixed IPMN) [5]. The anatomical classification is important since it dictates the malignant potential: MD-IPMN has a markedly higher risk of high-grade dysplasia (HGD)/invasive carcinoma (IC) than BD-IPMN [6]. These lesions show papillary proliferation, cyst formation, and varying degrees of cellular atypia [7].
Most patients are asymptomatic, and diagnosis is incidental when imaging studies are requested due to unrelated indications [8]. A small number may complain of nonspecific symptoms such as nausea, vomiting, abdominal or back pain, and others may have pancreatitis-like symptoms and develop exocrine and endocrine pancreatic insufficiency due to obstruction of the MPD by mucin. Therefore, in cases of acute or chronic pancreatitis we must exclude the presence of IPMN as an etiological factor, although differential diagnosis is challenging, especially in patients with Wirsung duct ectasia [9]. Due to the insidious nature and lack of awareness of the disease, there is often a delay in diagnosis of an IPMN in up to several months.
Since pancreatic cysts are common, the most important goal was to identify the small percentage of patients with high risk of developing a malignancy in the huge number of patients with presumed IPMNs, taking into account a healthcare economic perspective and the progressively older/frail population. For instance, 3.6 million dollars is spent on cyst surveillance for each cancer detected in the USA, without making appreciable change in cyst-related pancreatic adenocarcinoma mortality [10]. The increased detection and awareness of IPMNs led to the development of several consensuses and guidelines [5, 6, 11-13]. Although most of the data on IPMNs do not provide high-level evidence, the most recent guidelines are regarded as “evidence-based” [5, 11].
In this review, the Portuguese Pancreatic Club summarizes the risk assessment of a patient with an IPMN, focusing on the high-risk stigmata (HRSs)/ worrisome features (WFs) or absolute/relative indications for surgery according to different guidelines. An updated perspective on the surveillance strategy for IPMNs is presented comparing the available evidence. A literature review was performed using PubMed with the search terms “intraductal papillary mucinous neoplasm,” “surveillance,” and “follow-up.” The final manuscript was revised and approved by all members of the Governing Board of the Portuguese Pancreatic Club.
Risk Assessment
According to Fukuoka/Kyoto guidelines [5, 6], the predictive factors of HGD/IC in IPMNs have been called HRS/WF. Although HRSs are strong predictors of HGD/ IC, they lack specificity, which reinforces that other factors such as patient’s general condition, comorbidities, life expectancy, and preferences should be taken into account while addressing the decision of surgery [14]. The terms HRS/WF, used in Fukuoka/Kyoto consensus [5, 6], differ from the European guidelines, which consider instead the “absolute indication” and “relative indication” for surgery, as well as criteria for referral to multidisciplinary team meetings [11-13].
Table 1 compares HRS, absolute indications for surgery and for referral to multidisciplinary team meeting, according to the latest consensus and guidelines [5, 6, 11-13]. Obstructive jaundice is associated with HGD/IC with a sensitivity of 75-83% and a specificity of 61-65% [15]. Differentiating a mural nodule from a solid component is important since the former may indicate a noninvasive lesion and the last may point to IC or concomitant pancreatic ductal adenocarcinoma (PDAC). However, due to the difficulty in clinical practice to clearly distinguish them, both are considered HRS in the Fukuoka/Kyoto consensus. The cut-off value for the mural nodule (≥5 mm vs. ≥10 mm), as well as for the MPD dilation (≥5 mm vs. ≥10 mm), is still controversial [16]. Suspicious or positive cytology, if performed, may represent HGD/IC in 91-100% and 100%, respectively, but has low sensitivity [17].
Table 1 Indications for surgery (AGA institute guideline), absolute indications for surgery (European evidence-based guidelines), indications for referral to a multidisciplinary team meeting (ACG clinical guideline), and HRS (Kyoto guidelines) in a patient with IPMN
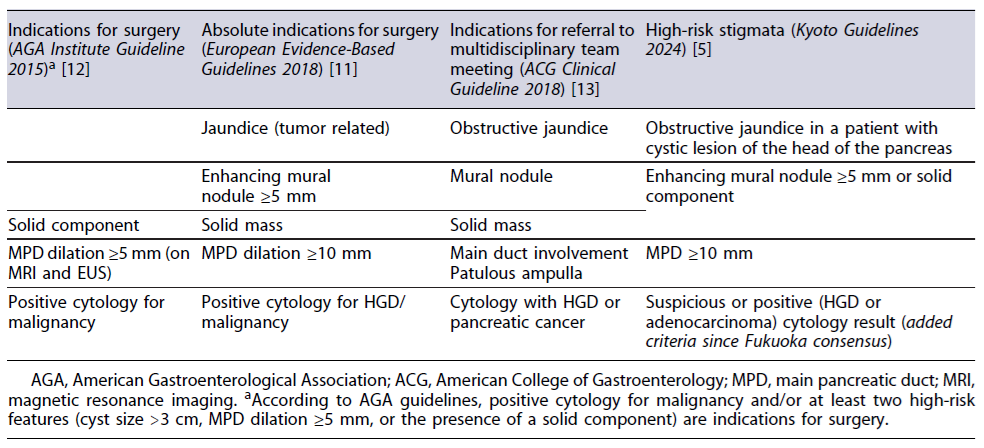
AGA, American Gastroenterological Association; ACG, American College of Gastroenterology; MPD, main pancreatic duct; MRI, magnetic resonance imaging. aAccording to AGA guidelines, positive cytology for malignancy and/or at least two high-risk features (cyst size >3 cm, MPD dilation ≥5 mm, or the presence of a solid component) are indications for surgery.
Table 2 compares the WF, relative indications for surgery and consideration for referral to multidisciplinary team meeting, according to the latest consensus and guidelines [5, 6, 11-13]. As previously stated, the MPD obstruction due to viscous mucin secretion or MPD stenosis due to tumor involvement may cause acute pancreatitis, reported in up to 20% of patients with an IPMN [12]. However, larger series have pointed out that incidence of HGD/IC for patients with IPMNs and history of acute pancreatitis is similar in patients with IPMNs and low-grade dysplasia [18]. In case of repeated episodes of acute pancreatitis, surgery may be considered to improve quality of life [5]. Increased CA 19-9 is considered a good predictor of malignancy including PDAC and IPMN with HGD/IC and should prompt consideration for surgical therapy [19]. However, the current CA 19.9 cut-off was recently demonstrated to shorten surveillance intervals, cause unnecessary surgeries, and is not predictive of HGD/ IC [20]. New onset/recent exacerbation of diabetes mellitus carries increased risk of HGD/IC and should be considered a WF according to Kyoto and European guidelines, highlighting the importance of HbA1c in surveillance [5, 11]. Thickened cyst walls, although without an evidenced-based cut-off to predict HGD/IC (one report proposed a 2.5-mm cut-off, with an odds ratio of 3.51 [21]), abrupt change in caliber of MPD with distal atrophy, lymphadenopathy, and cyst growth ≥2.5 mm/ year are considered WFs (the last criteria changed with the recent guidelines vs. ≥5 mm/2 years in 2017 Fukuoka guidelines). It is worth mentioning that the greater the number of risk factors, the higher the probability of malignancy [22]. Indeed, the risk of HGD/IC increases in a stepwise fashion with the number of WF to 22, 34, and 59% with 1, 2, and 3 WF, respectively, reaching 100% in patients with 4 or more WF [5].
Table 2 Relative indications for surgery (European evidence-based guidelines), consideration for referral to a multidisciplinary team meeting (ACG clinical guideline) and worrisome features (Kyoto guidelines) in a patient with IPMN
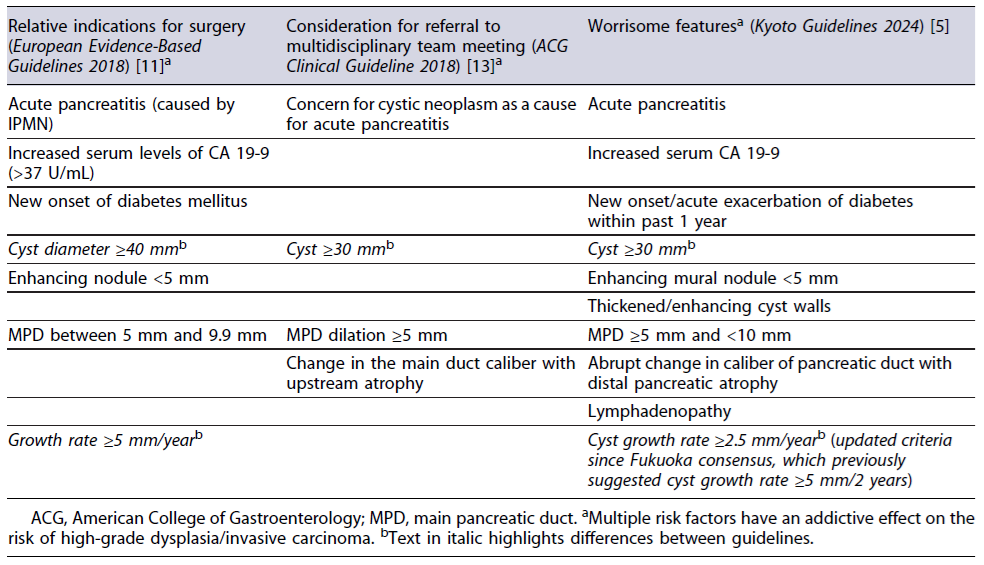
ACG, American College of Gastroenterology; MPD, main pancreatic duct. aMultiple risk factors have an addictive effect on the risk of high-grade dysplasia/invasive carcinoma. bText in italic highlights differences between guidelines.
As stated before, MD-IPMNs carry a higher risk for malignant transformation and surgical fit patients should be referred for surgery. Since mixed-type IPMNs may behave in a similar fashion as MD-IPMNs, the same principle applies and patients should also be referred for surgery [5, 11]. Preoperative counseling is essential discussing surgical options with the patient ranging from radical pancreatectomy with lymphadenectomy if IC is suspected to organ-preserving techniques if noninvasive lesion is considered [5].
Surveillance of Non-Resected IPMNs
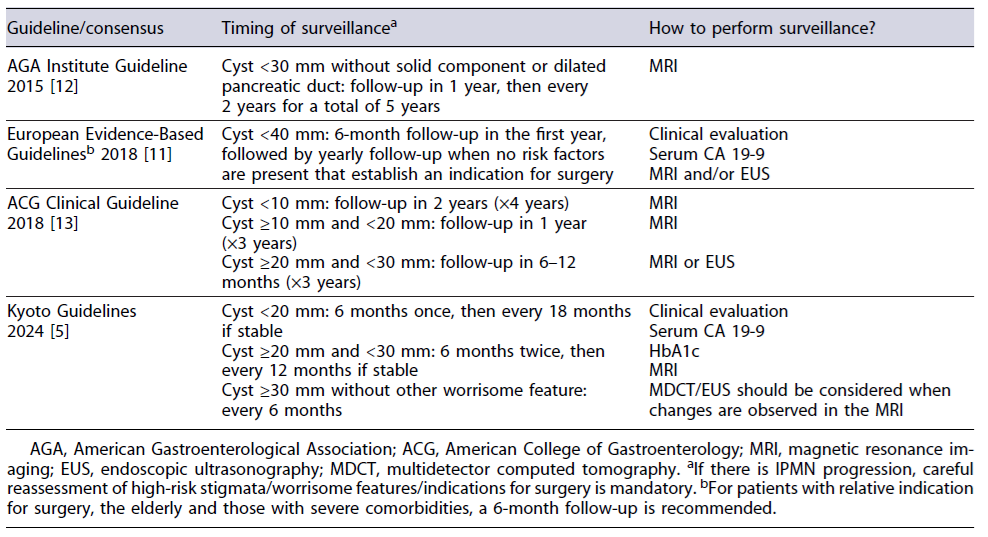
The “dual carcinogenesis” is a key concept during management of IPMNs, as cancer may occur either from progression of IPMN to HGD/IC (IPMN-derived car-cinoma) or from development of PDAC apart from IPMN in the same pancreas (concomitant PDAC). In non-resected IPMNs, clinicians should bear in mind that cumulative incidence of transformation of indolent BD- IPMN to HGD/IC is 0.94-3.3% by 5 years, 2.3-6.6% by 10 years, and 7.6-15% by 15 years [5], although the risk is lower than previously considered [23]. The most important risk factors for IPMN-derived carcinoma are cyst size and MPD diameter at diagnosis, although these factors were not associated with the risk of concomitant PDAC [24]. Table 3 highlights the surveillance strategy for the non-resected IPMNs according to the latest consensus and evidence-based guidelines, regarding timing and the proposed method [5, 6, 11-13].
Table 3 Surveillance strategy for the non-resected IPMN according to the latest consensus and guidelines
Multifocal BD-IPMNs are reported in around 20-40% of the patients [6], and the majority of these lesions arise independently (“field defect theory”). Multifocality is not a criterion for considering increased risk for HGD/IC [25, 26]. In this regard, management should be dictated by the lesion having the highest risk, either if indication for surgery or surveillance [5].
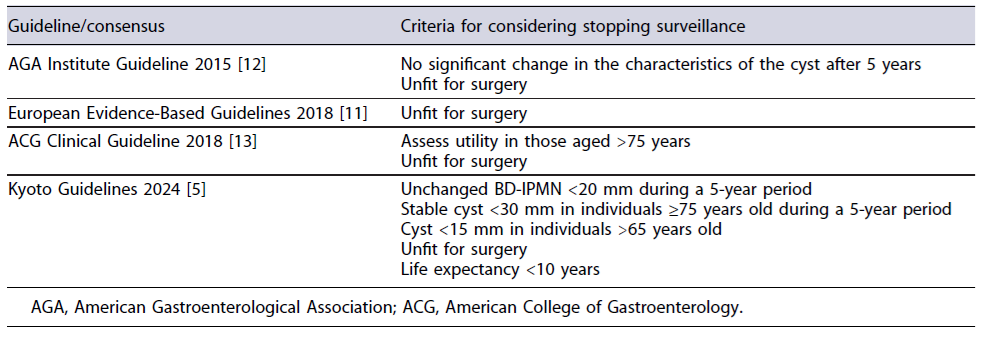
One important aspect of non-resected IPMNs is when clinicians should/may stop surveillance. Life-long surveillance is associated with a significant healthcare expenditure and psychological burden for the patient/ physician [27]. Although finding appropriate criteria to decide surveillance discontinuation is important, clinicians should bear in mind that risk of concomitant PDAC remains even after a 5-year follow-up [28]. The risk of concomitant PDAC is about 3- to 5-fold higher comparing with age-matched population [28], and all these facts must be discussed with the patient before deciding to stop surveillance. Moreover, some patients with contraindications for surgery may be considered candidates for endoscopic ultrasonography-guided ablation therapy, and this might influence the decision to continue/stop surveillance [29]. Table 4 includes proposed criteria to consider stopping surveillance, according to different guidelines/consensuses. Ideally, surveillance of presumed BD-IPMN should be safely discontinued in selected patients once their risk of malignancy is similar to the risk of age-matched general population [23].
Extra-Pancreatic Neoplasms
In patients with IPMNs, extra-pancreatic neoplasms are reported in up to 30% [5]. Most of them are diagnosed during initial assessment or after resection of extra-pancreatic neoplasms, but in the remaining patients, extra-pancreatic neoplasms may be diagnosed during IPMN surveillance [30]. The distribution of involved organs depends on ethnicity and country. In the Western world, skin, breast, kidney, and prostate are frequent malignancies associated with IPMN, in contrast with Asian countries, with a higher prevalence of gastrointestinal cancers [31]. Despite this, recent evidence suggests that incidence of extra-pancreatic neoplasms in patients with IPMNs is similar compared with population-based incidence of each country [32]. No additional screening besides the national protocols regarding extra-pancreatic neoplasms is necessary in patients with IPMNs.
Comparison between Guidelines
As previously stated, there are several published national and international guidelines, mainly consensus based. Currently, the 2015 American Gastroenterological Association (AGA) [12], the 2018 European Study Group on Cystic Tumors of the Pancreas [11], the 2018 American College of Gastroenterology (ACG) [13], and the 2024 International Association of Pancreatology (IAP) [5] provide recommendations on follow-up concerning the risk of malignancy.
Due to the complex and indolent nature of the disease, the primary goal when discussing IPMN surveillance is to find the balance between the risk of malignant progression and overtreatment. Tables 1-3 highlight small but important differences concerning high-risk features for HGD/IC, timing and method of surveillance, as well as factors that may result in follow-up discontinuation.
For IPMNs, the IAP and European guidelines suggest resection when the MPD is involved (MPD ≥10 mm; or in cases of mixed-type IPMN). In contrast, according to AGA recommendations, the presence of a mural nodule or positive cytology for malignancy is a necessary condition. Management of BD-IPMN differs between guidelines, raising concerns about which one has the better diagnostic accuracy.
In a monocentric retrospective cohort, the AGA 2015/ IAP 2017/European Guidelines 2018 were compared to evaluate the diagnostic accuracy in identifying advanced neoplasia in patients with IPMNs [33]. The AGA guidelines were found to have a lower sensitivity (27%), with the risk of missing advanced neoplasia in 26%, compared with 2.1% and 1.4% with the IAP and European recommendations, respectively. In this regard, the IAP and European guidelines are associated with higher rates of unnecessary surgery (83% and 76%) against 8.6% in the AGA recommendations. Other studies have demonstrated a missed rate of advanced neoplasia in 12-93% when applying the AGA guidelines [34-36]. Considering the 2017 IAP guidelines, the HRS was associated with 90% sensitivity and 67% specificity for identifying advanced neoplasia in IPMN [37]. One multicenter study demonstrated that the accuracy of the 2018 European guideline was 65% when ≥1 relative indication was present [38]. Due to the novelty of the Kyoto guidelines from 2024 [5], no study has so far assessed the diagnostic accuracy in detecting advanced neoplasia in IPMNs.
From the authors’ perspective, we tend to follow the IAP guidelines with the definition of HRS/WF to guide for resection, to maintain surveillance according to the cyst size or to consider discontinuing follow-up if criteria proposed by the same group are met. However, clearly new diagnostic approaches are needed to more accurately identify high-risk patients. Next-generation sequencing of cyst fluid, with some promising results [39], multi-modality tests that evaluate clinical features, imaging characteristics, genetic and biochemical markers [40], or even artificial intelligence-based clinical decision-making [41] may complement our clinical practice with the aim of improving future outcomes.
Conclusions/Key Points
Most of the current guidelines have a low malignancy miss rate with the cost of surgical overtreatment.
According to 2024 Kyoto Guidelines, the HRS and WF should be searched as potential indications for surgery, especially if multiple WFs are present.
Surveillance of a non-resected IPMN depends on the cyst size and is mainly performed with clinical evaluation, CA 19-9, HbA1c, and magnetic resonance imaging; endoscopic ultrasonography should be considered if there are changes in other imaging methods, especially if fine-needle aspiration may modify management.
Multidisciplinary management preferably in reference centers is of utmost importance given the indolent and complex nature of the disease.
A global evidence-based guideline that combines the several guideline groups is mandatory to uniformize care.

