










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Public Health
versão impressa ISSN 2504-3137versão On-line ISSN 2504-3145
Port J Public Health vol.36 no.1 Lisboa 2018
https://doi.org/10.1159/000486014
RESEARCH ARTICLE
Trends in Portuguese Adolescents’ Sexual Behavior from 2002 to 2014: HBSC Portuguese Study
Comportamento sexual dos adolescentes portugueses entre 2002 e 2014: estudo de HBSC em português
Marta Reis a, b , Lúcia Ramiro a,b , Inês Camacho a, b Gina Tomé a, b Margarida Gaspar de Matos a,b,c
a Projeto Aventura Social & Saúde, Faculdade de Motricidade Humana, Universidade de Lisboa, Lisbon, Portugal
b Instituto de Saúde Ambiental (ISAMB), Faculdade de Medicina, Universidade de Lisboa, Lisbon, Portugal
c William James Research Center, ISPA – Instituto Superior de Psicologia Aplicada, Lisbon, Portugal
ABSTRACT
This study examined trends in adolescent sexual behaviors from 2002 to 2014 in Portugal. Data were collected using self-reported questionnaires from 8th and 10th graders in classrooms during 2002, 2006, 2010, and 2014. Overall, the prevalence of sexual intercourse, age of sexual initiation, pill use, and sexual intercourse under the influence of alcohol or drugs decreased in Portugal between 2002 and 2014, while condom use increased. Boys and 10th graders more frequently reported having ever had sexual intercourse, boys and 8th graders more frequently reported having had sexual intercourse under the influence of alcohol or drugs, girls and 10th graders more frequently reported having had their first sexual intercourse at 14 years or older (except in 2014, where boys and girls reported more frequently having initiated at 12–13 years), and girls and 10th graders reported more frequently having used condoms and the pill (except in 2014) at the last sexual intercourse. Eighth graders more frequently reported having had their first sexual experience at 12–13 years (except in 2006).
Keywods: Adolescents Sexual experience Age of sexual initiation Condom use Pill use Sexual intercourse under the influence of alcohol or drugs
RESUMO
Este estudo examinou as tendências dos comportamentos sexuais de adolescentes de 2002 a 2014 em Portugal. Os dados foram recolhidos usando questionários de autorrelato nos alunos de 8° e 10° anos de escolaridade, nas salas de aula durante 2002, 2006, 2010 e 2014. Em geral, a prevalência de relações sexuais, a idade de iniciação sexual, o uso da pílula e as relações sexuais sob a influência de álcool ou drogas diminuiu em Portugal entre 2002 e 2014, enquanto o uso de preservativos aumentou. Os rapazes e os alunos do 10° ano referiram mais frequentemente terem tido relações sexuais, os rapazes e os alunos do 8° ano mencionara ter tido, mais frequentemente relações sexuais sob a influência de álcool ou drogas, as raparigas e os alunos do 10° ano relataram mais frequentemente terem tido sua primeira relação sexual aos 14 ou mais (exceto em 2014, onde rapazes e raparigas referiram mais frequentemente ter iniciado às 12–13), e as raparigas e os alunos do 10° ano relataram mais frequentemente ter usado preservativo e pílula (exceto em 2014) na última relação sexual. Os alunos do 8° ano referiram mais frequentemente terem tido sua primeira experiência sexual aos 12–13 (exceto em 2006).
Palavras chave: Adolescentes · Experiência sexual · Idade de iniciação sexual · Uso de preservativo · Uso da pílula · Relações sexuais sob a influência de álcool ou drogas
Introduction
Adolescents, unlike adults, may be more prone to engage in risky sexual behavior due to perceptions of personal invulnerability and their tendency to focus on the immediate, rather than long-term, consequences of their behavior ( 1 - 3 ). The majority of older adolescents (aged 15 years or older) in Portugal are sexually active, yet many do not take appropriate precautions to prevent preg nancy or the spread of sexually transmitted infections (STIs) 3.
Adolescents routinely engage in behaviors that put their health at risk. Risky sexual behaviors are of particular concern to parents, teachers, and health professionals in that they can lead to serious consequences both for the adolescents involved and for any number of unseen partners. Parents, teachers, and health professionals are faced with 3 challenges: (1) how to understand this behavior, (2) how to identify risky sexual behavior in the adolescent, and (3) what to do about it.
Age of sexual initiation has been decreasing in several industrialized countries ( 1 , 3 , 4 ). According to recent Health Behaviour in School-Aged Children (HBSC) surveys, most sexually active 15-year-olds reported having had their first sexual intercourse from 14 years of age upwards ( 5 , 6 ). Addressing sexual behavior among very young people is therefore of significant relevance to public health ( 7 - 9 ).
Sexual activity is commonly initiated during adolescence ( 1 - 3 ), but while generally accepted as a normative part of the transition to adulthood, it can have negative consequences such as infection with HIV and other STIs, unwanted pregnancy, and abortion. Young people are at higher risk of related negative outcomes than adults, primarily due to their relative physical, emotional, and cognitive immaturity ( 10 , 11 ), and tend to engage more frequently in risky behaviors such as sexual intercourse without a condom ( 2 , 12 , 13 ). Recent data suggest that among adolescents in Western, Central, and Eastern Europe 1 who have had intercourse, up to 40% had not used condoms during their last sexual intercourse; thus, many sexually active adolescents remain at risk of infection by HIV and other STIs. Although there has been a recent decline in HIV infection among adolescents in industrialized countries, rates of other STIs have increased ( 1 , 4 , 14 ).
This paper aims to (1) describe trends in sexual experience, sexual initiation, condom and pill use at the last sexual intercourse, and sexual intercourse under the influence of alcohol or drugs among adolescents of the 8th and 10th grades from 2002 to 2014 in Portugal; and (2) describe variations in these trends over time in boys and girls and school grades (8th and 10th).
Methods
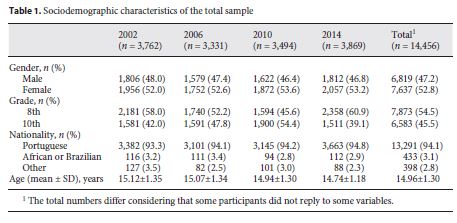
Data were collected through a self-administered questionnaire from the Portuguese sample of the HBSC study of 2002, 2006, 2010, and 2014 ( 15 - 16 ). The study provided national representative data of 14,456 Portuguese adolescents, randomly chosen from those attending the 8th and 10th grades of high school and the opportunity to examine trends in sexual behavior. The sample included 52.8% girls and 47.2% boys, whose mean age was 14.96 years (SD = 1.30). The majority was of Portuguese nationality (94.1%); 54.5% attended the 8th grade and 45.5% the 10th grade (Table 1 ).
The sampling unit used in this survey was the class. The schools in the sample were randomly selected from the official national list of public schools. In each school, classes were randomly selected in order to meet the required number of students for each grade, according to the international research protocol.
This study was approved by a scientific committee, an ethical national committee, and the national commission for data protection and strictly followed all the guidelines for human rights protection.
In the questionnaire, which covered a wide range of questions about behaviors and lifestyles in adolescence, issues were selected that relate to sociodemographic characteristics and sexual behavior 17.
Measures
Sexual Behaviors
Experience of sexual intercourse was assessed by the question “Have you ever had sexual intercourse?” (Yes/No); age of first sexual intercourse by “How old were you when you had sexual intercourse for the first time?” (11 or younger/12/13/14/15/16/17 or older; in the 2014 survey the option “17 or older” was withdrawn and the last option was “16 or older”). Responses were dichotomized into “11 or younger,” “12–13 years,” and “14 or older.” Condom use, pill use, and having had sexual intercourse under the influence of alcohol or drugs were assessed by the following questions: “The last time you had sexual intercourse, did you or your partner use a condom?,” “The last time you had sexual intercourse, did you or your partner use a pill?,” and “Have you ever had sexual intercourse under the influence of alcohol or drugs?” (Yes/No). In the last survey (2014), the question about condom and pill use had 3 answer options – Yes/No/I do not know. Those who answered “I do not know” to either of the 2 items were coded as not having used a condom or the pill at the last intercourse, respectively.
Time was included as a ratio variable reflecting the year of study with 2002 as baseline.
Statistical Analyses
Analyses and statistical procedures were carried out in the Statistical Package for Social Sciences program (version 22 for Windows). Overall, 14,456 participants completed structured self-reported questionnaires. The total numbers differed considering that some participants did not reply to some questions. Descriptive statistics were performed to characterize the sample and to examine sexual behaviors according to gender and grade. χ 2 analyses were used to examine sexual behaviors. Upward or downward trends were determined through the comparison of the module that corresponded to an adjusted residual ≥|1.9|. The level for statistical significance was set at p < 0.001.
Results
Differences between 2002, 2006, 2010, and 2014 for questions about sexual behaviors
Table 2 shows the trends in sexual behaviors between 2002 and 2014. There was a statistically significant difference in the percentage of participants reporting ever having had sexual intercourse (χ 2 (3) = 75.578, p ≤ 0.001). There was a significant decrease from 2002 to 2014.
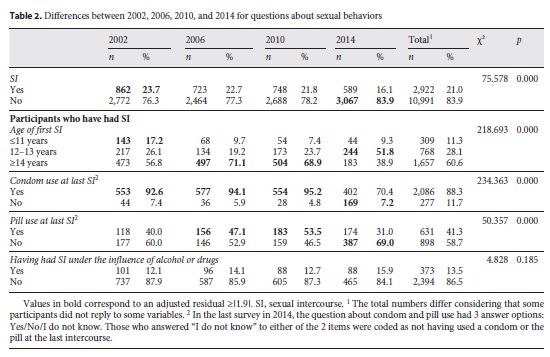
Among those who were sexually active, regarding the age of first sexual intercourse of 14 years or older, an overall decrease was observed (χ 2 (3) = 218.693, p ≤ 0.001), with rates ranging from 38.9% (2014) to 71.1% (2006). Moreover, according to the results of the last study, participants most frequently reported having had sexual intercourse for the first time at the age of 12–13 years.
Among those who were sexually active, overall, 88.3% reported that they or their partner had used a condom the last time they had engaged in sexual intercourse, which means that about 12% are currently at high risk. Considering the 4 cycles of the study, an increase was observed (χ 2 (3) = 234.363, p ≤ 0.001), which was especially strong between 2002, 2006, and 2010, and a decrease was observed from 2010 to 2014.
Regarding those who were sexually active, overall, only 41.3% reported that they or their partner had used the pill the last time they had engaged in sexual intercourse. Considering the 4 cycles of the study, an increase was observed (χ 2 (3) = 50.357, p ≤ 0.001), which was especially strong between 2006 and 2010, and a decrease was observed from 2010 to 2014.
There was no statistically significant difference for having had sexual intercourse under the influence of alcohol or drugs (χ 2 (3) = 4.828, p = 0.185).
Differences between 2002, 2006, 2010, and 2014 and Gender for Questions about Sexual Behaviors
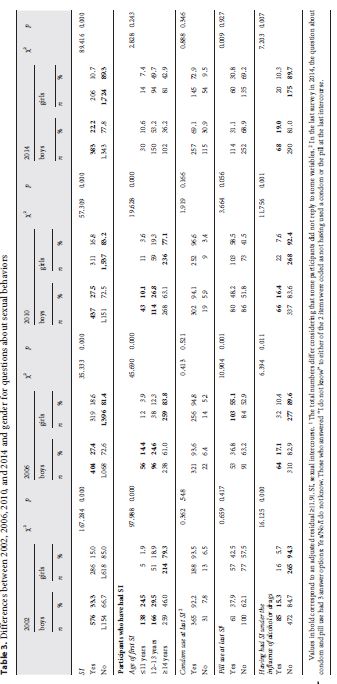
Table 3 shows the trends in sexual behaviors between 2002 and 2014 by gender. There was a statistically significant difference by gender between participants reporting having ever had sexual intercourse in the 4 cycles of the study, with boys reporting more frequently having had sexual intercourse than girls (χ 2 (1) = 167.284, p ≤ 0.001; χ 2 (1) = 35.333, p ≤ 0.001; χ 2 (1) = 57.309, p ≤ 0.001; χ 2 (1) = 89.416, p ≤ 0.001). In addition, results suggested that there was a significant decrease in the rate of boys who reported having had sexual intercourse from 2002 to 2014.
Among those who were sexually active, an overall increase was observed regarding age of first sexual intercourse between boys and girls, especially in 2002, 2006, and 2010 (χ 2 (1) = 97.988, p ≤ 0.001; χ 2 (1) = 45.690, p ≤ 0.001; χ 2 (1) = 19.628, p ≤ 0.001), peaking in 2006, with girls mentioning more frequently than boys to have had sexual intercourse at the age of 14 years or older. There was no statistically significant difference between gender and the age of first sexual intercourse in 2014. Nevertheless, results showed that both boys and girls more frequently reported having had their first sexual intercourse at the age of 12–13 years, particularly boys.
There was no statistically significant difference between boys and girls as for the use of a condom the last time they had engaged in sexual intercourse for the 4 cycles of the study and for the use of the pill in 3 cycles of the study (2002, 2010, and 2014). In 2006, girls reported more frequently having used the pill the last time they had engaged in sexual intercourse. Although not representing statistically significant differences, overall results showed that girls more often than boys reported having used a condom and the pill at the last sexual intercourse.
Regarding those who were sexually active, statistically significant differences were observed between boys and girls, which showed an increasing trend with boys reporting more often having had sexual intercourse under the influence of alcohol or drugs in the 4 cycles of the study (χ 2 (1) = 16.125, p ≤ 0.001; χ 2 (1) = 6.394, p ≤ 0.050; χ 2 (1) = 11.756, p ≤ 0.001; χ 2 (1) = 7.203, p ≤ 0.010).
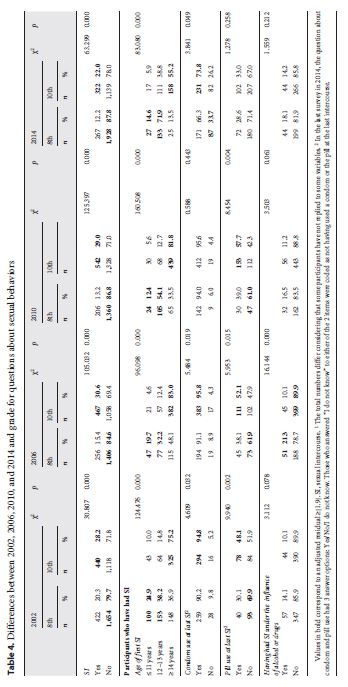
Differences between 2002, 2006, 2010, and 2014 and Grade for Questions about Sexual BehaviorsTable 4 shows the trends in sexual behaviors between 2002 and 2014 by grade. There was a statistically significant difference between 8th and 10th graders who reported having ever had sexual intercourse in the 4 cycles of the study, with the students of the 10th grade reporting more frequently having had sexual intercourse. In addition, the number of 8th graders who reported having ever had sexual intercourse decreased from 2002 to 2014 (χ 2 (1) = 30.807, p ≤ 0.001; χ 2 (1) = 105.032, p ≤ 0.001; χ 2 (1) = 125.397, p ≤ 0.001; χ 2 (1) = 63.299, p ≤ 0.001); therefore, a decreasing trend is noticeable.
Among those who were sexually active, an overall increase was observed in age of first sexual intercourse among 10th graders who reported having had sexual intercourse at the age of 14 years or older, from 2002 to 2010, peaking in 2006; whereas in 2014, a decrease was noticeable (χ 2 (1) = 124.476, p ≤ 0.001; χ 2 (1) = 96.098, p ≤ 0.001; χ 2 (1) = 160.508, p ≤ 0.001; χ 2 (1) = 83.080, p ≤ 0.001). There were statistically significant differences for 3 cycles of the study (2002, 2006, and 2014) between 8th and 10th graders reporting the use of a condom the last time they had engaged in sexual intercourse, with the students of the 10th grade reporting using a condom more frequently than the students of the 8th grade (χ 2 (1) = 4.609, p ≤ 0.050; χ 2 (1) = 5.484, p ≤ 0.050; χ 2 (1) = 3.841, p ≤ 0.050). There was no statistically significant difference between grade and the use of a condom the last time participants had engaged in sexual intercourse in 2010.
Among those who were sexually active, statistically significant differences between grades were observed regarding the use of the pill at the last sexual intercourse for 3 cycles of the study (2002, 2006, and 2010), with the students of the 10th grade reporting an overall increase in comparison to the students of the 8th grade (χ 2 (1) = 9.940, p ≤ 0.010; χ 2 (1) = 5.953, p ≤ 0.050; χ 2 (1) = 8.454, p ≤ 0.010). There was no statistically significant difference between grades and the use of the pill at the last sexual intercourse in 2014. In 2014, both 8th and 10th graders’ pill use at the last sexual intercourse decreased.
Regarding those who were sexually active and reported having had sexual intercourse under the influence of alcohol or drugs, statistically significant differences were observed between grades only in 2006, with the students of the 8th grade reporting to have had sexual intercourse under the influence of alcohol or drugs more frequently than the students of the 10th grade (χ 2 (1) = 16.144, p ≤ 0.001). There were no statistically significant differences for having had sexual intercourse under the influence of alcohol or drugs between grades in 2002, 2010, and 2014. It was also noticeable that both 8th and 10th graders reported more frequently having had sexual intercourse under the influence of alcohol or drugs in 2014.
Discussion
The goal of this study was to document recent trends in preventive sexual behaviors in Portuguese adolescents and assessing whether they have changed and how they have changed from 2002 to 2014.
Comparing the data from the 2002, 2006, 2010, and 2014 surveys, results showed an increasing trend regarding the percentage of participants reporting their first sexual intercourse at 14 years or older (except in 2014) and condom use at the last sexual intercourse (except in 2014) as well as a stabilized trend concerning having had sexual intercourse, pill use at the last intercourse (except in 2014), and having had intercourse under the influence of alcohol or drugs.
Overall, in terms of differences between gender and grade, results showed that boys and older adolescents (10th graders) more often stated having had sexual intercourse. Girls and 8th graders more often reported having had their first sexual intercourse at 14 years or older, and 10th graders more often reported having used a condom and/or the pill during their last sexual intercourse. Condom use among sexually active adolescents has been increasing over the same period, especially so among girls.
In terms of the latest survey, specifically, on the one hand, there was an improvement in sexual reproductive health because some preventive behaviors have either increased (having ever had sexual intercourse) or stabilized (having had sexual intercourse under the influence of alcohol or drugs). On the other hand, some results suggested that some sexual risk behaviors may be increasing since the age of first sexual intercourse may be decreasing to 12–13 years, and condom and pill use at the last sexual intercourse may be decreasing.
Although these results may seem significant, they must be interpreted with caution. They may suggest an inversion of the trends from 2002 to 2010, but it is not possible to attest to it yet. It would be of great interest to compare these results with those of other HBSC countries. They may be the result of the reduction of investment that has been put into sexual education since the 2010 survey, when the Ministry of Education stopped putting schools under pressure concerning sexual education; they may be due to the latest scientific developments concerning AIDS; or they may reflect innumerous reasons not accounted for in this paper.
Regardless of potentially worrisome results, the authors must recall that the 2014 survey results are overall positive in terms of sexual health, suggesting that the majority of those who attend the 8th and 10th grades do have protective behaviors.
Nevertheless, in addition to overall protective results (including 2014), a significant minority of adolescents is involved in risk behaviors such as not having used a condom at the last sexual intercourse and having had sex at 13 years or younger, behaviors that can bring major negative outcomes individually and in terms of public health ( 3 , 8 , 9 , 18 ).
Past analyses (from 2002 to 2010) suggested that formal sexual education in the school context promoted protective sexual behaviors 19; therefore, it must be determined whether sexual education has been modified or interrupted. In other words, sexual education in the school context should be evaluated.
In 2013, an evaluation about the implementation of the law No. 60/2009 (6th August) 20 on sexual education in schools was carried out. The results showed that the law was being fulfilled and, in general, the schools organized an office that provided information and support for students and managed its functioning. In addition, school principals and teachers emphasized that schools were making a huge effort to implement the law. However, some of them questioned their ability to continue this process due to the economic restrictions at the time. Principals and teachers reported the need to “revitalize” this area, underlining the need to maintain the law and one annual “Call” from which the Ministry of Education and Science received proposals for funding schools for projects in the area of health promotion as well as teacher training 21.
It is crucial to understand if and why prevention strategies have not been as successful overall as they seemed to have been in the past.
In conclusion, it is important to highlight adolescents’ reported adoption of preventive behaviors, but also how these have been changing from 2002 to 2014, which demands for careful monitoring.
NOTES
1 Avery L, Lazdane G: What do we know about sexual and reproductive health of adolescents in Europe? Eur J Contracept Reprod Health Care 2010; 15:S54–S66.
2 WHO: A Snapshot of the Health of Young People in Europe. Copenhagen, WHO Regional Office for Europe, 2011. [ Links ]
3 Ramiro L, Windlin B, Reis M, Gabhainn SN, Jovic S, Matos MG, et al: Trends in very early sex and condom use in 20 European countries from 2002 to 2010. Eur J Public Health 2015; 25(suppl 2):65–68.
4 Wellings K, Collumbien M, Slaymaker E, Susheela S, Hodges Z, Patel D, et al: Sexual behaviour in context: a global perspective. Lancet 2006; 368: 1706–1728.
5 Nic Gabhainn S, Baban A, Boyce W, Godeau E; HBSC Sexual Health Focus Group: How well protected are sexually active 15-year olds? Cross-national patterns in condom and contraceptive pill use 2002–2006. Int J Public Health 2009; 54(suppl 2):209–215.
6 Currie C, Zanotti C, Morgan A, Currie D, de Looze M, Roberts C, et al: Social determinants of health and well-being among young people; in WHO: Health Behaviour in School-Aged Children (HBSC) Study: International Report from the 2009/2010 Survey. Copenhagen, WHO Regional Office for Europe, 2012. [ Links ]
7 Kaestle CE, Halpern CT, Miller WC, Ford CA: Young age at first sexual intercourse and sexually transmitted infections in adolescents and young adults. Am J Epidemiol 2005; 161: 774–780.
8 Santelli JS, Lindberg LD, Finer LB, Singh S: Explaining recent declines in adolescent pregnancy in the United States: the contribution of abstinence and improved contraceptive use. Am J Public Health 2007; 97: 150–156.
9 Anderson JE, Santelli JS, Morrow B: Trends in adolescent contraceptive use, unprotected and poorly protected sex, 1991–2003. J Adolesc Health 2006; 38: 734–739.
10 UNAIDS: Joint United Nations Programme on HIV/AIDS: Global AIDS Update 2016. Geneva, Joint United Nations Programme on HIV/AIDS, UNAIDS, 2016. [ Links ]
11 Godeau E, Vignes C, Duclos M, Navarro F, Cayla F, Grandjean H: Facteurs associés à une initiation sexuelle précoce chez les filles: données Françaises de l’enquête internationale Health Behaviour in School-Aged Children (HBSC)/OMS. Gynecol Obstet Fertil 2008; 36: 176–182.
12 UNAIDS: Global Report: UNAIDS Report on the Global AIDS Epidemic 2010. Geneva, Joint United Nations Programme on HIV/AIDS, UNAIDS, 2010. [ Links ]
13 UNAIDS: Report on the Global HIV/AIDS Epidemic 2008. Geneva, Joint United Nations Programme on HIV/AIDS, UNAIDS, 2008. [ Links ]
14 Fenton KA, Lowndes CM; the European Surveillance of Sexually Transmitted Infections (ESSSTI) Network: Recent trends in the epidemiology of sexually transmitted infections in the European Union. Sex Transm Infect 2004; 80: 255–263.
15 Matos MG, Simões C, Tomé G, Camacho I, Ferreira M, Ramiro L, et al: A saúde dos adolescentes portugueses: Relatório do Estudo HBSC 2010. ACS/FMH/UTL/CMDT-UNL, 2011.
16 Matos MG, Simões C, Camacho I, Reis M; Equipa Aventura Social: A saúde dos adolescentes portugueses em tempos de recessão: dados nacionais de 2014: Relatório final do Estudo HBSC 2014. Lisbon, Centro Malária e Outras Doenças Tropicais, IHMT, UNL, FMH, Universidade de Lisboan 2015. [ Links ]
17 Roberts C, Currie C, Samdal O, Currie D, Smith R, Maes L: Measuring the health and health behaviours of adolescents through cross-national survey research: recent developments in the Health Behaviour in School-aged Children (HBSC) study. J Public Health 2007; 15: 179–186.
18 Wellings K, Nanchahal K, Macdowell W, McManus S, Erens B, Mercer C, et al: Sexual behaviour in Britain: Early heterosexual experience. Lancet 2001; 358: 1843–1850.
19 Ramiro L, Reis M, Matos MG, Diniz JA: Sex education among Portuguese adolescent students. Procedia Soc Behav Sci 2011; 29: 493–502.
20 Lei n° 60/2009. D.R. I Série. 151 (2009/08/06) 5097–5098.
21Matos MG, Reis M, Ramiro L, Ribeiro JLP, Leal I: Sexual education in schools in Portugal: evaluation of a 3 years period. Creat Educ 2014; 5: 1353–1362.
Acknowledgements
The authors are grateful to the Team Social Adventure, Faculty of Human Kinetics, University of Lisbon, to all participants, and to the Foundation for Science and Technology, Ministry of Science and Higher Education.


{kind=link}
{kind=link}