










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Public Health
versão impressa ISSN 2504-3137versão On-line ISSN 2504-3145
Port J Public Health vol.36 no.2 Lisboa 2018
https://doi.org/10.1159/000492084
RESEARCH ARTICLE
Measuring Empowerment in Patients with Chronic Disease: Psychometric Qualities of the Portuguese Rheumatic Disease Empowerment Scale
Avaliação do empowerment em pacientes com doença crónica: Qualidades psicométricas da Escala Portuguesa de Empowerment na Doença Reumática
Marta Pereira Alves a Ana Isabel Cunha b Tatiana Lopes b Pedro Abreu c Cláudia Vaz d
a Research Center in Business Sciences (NECE-UBI)/Departamento de Psicologia e Educação, Universidade da Beira Interior, Covilhã, Portugal
b Departamento de Psicologia e Educação, Universidade da Beira Interior, Covilhã, Portugal
c Unidade Local de Saúde de Castelo Branco, E.P.E., Unidade de Reumatologia, Castelo Branco, Portugal
d Unidade Local de Saúde da Guarda, E.P.E., Serviço de Reumatologia, Guarda, Portugal -
ABSTRACT
Empowerment is usually defined as a process of promoting the sense of competence and control as a means of capacitating individuals to improve their life conditions. The aim of this study was to describe the psychometric qualities of the Portuguese Rheumatic Disease Empowerment Scale (P-RES-8), an 8-item measure of empowerment for patients with rheumatic disease. The study enrolled 81 patients with rheumatic diseases. Participants filled in the P-RES-8, the Portuguese validated version of the Medical Outcomes Survey Short Form-36 (MOS SF-36), and a questionnaire including sociodemographic data and disease-related variables. To evaluate the dimensionality of the P-RES-8 scale, an exploratory factor analysis was conducted, and its reliability was assessed by Cronbach’s α. The validity of this measure was assessed by analyzing the correlations between empowerment, quality of life, and other relevant variables (education level and illness duration). The P-RES-8 proved to be a reliable 1-dimensional measure of empowerment in patients with rheumatic disease (Cronbach’s α = 0.94). Empowerment was positively related to quality of life. Particularly, the findings showed positive associations between empowerment, assessed by the P-RES-8, and each of the 8 domains of the MOS SF-36. The associations were stronger for mental health and general health perception. The results also revealed that empowerment is positively associated with a higher education and more years after the diagnosis. The findings provide support for the adequacy of the P-RES-8 as a measure of empowerment in patients with rheumatic disease. Moreover, empowerment showed to be an important variable in the assessment of patients’ quality of life.
Keywords: Chronic disease empowerment Rheumatic diseases Psychometrics Quality of life Health psychology -
RESUMO
O empowerment é geralmente definido como um processo de promoção da perceção de competência e de controlo como forma de capacitar os indivíduos para melhorar suas condições de vida. O estudo teve como objetivo analisar as qualidades psicométricas da Escala Portuguesa de Empowerment na Doença Reumática (P-RES-8), uma medida constituída por 8 itens destinada a pacientes com doença reumática. O estudo envolveu 81 sujeitos com doenças reumáticas. Os participantes preencheram o PRES- 8, a versão validada em português do Medical Outcomes Survey Short Form-36 (MOS SF-36) e um questionário de avaliação de dados sociodemográficos e variáveis relacionadas com a doença. Para avaliar a estrutura dimensional da escala P-RES-8, foi realizada uma análise fatorial exploratória, e a sua consistência foi avaliada através do cálculo do alfa de Cronbach. A validade desta medida foi avaliada através da análise das correlações entre empowerment, qualidade de vida e outras variáveis relevantes (nível de escolaridade e tempo de duração da doença). A P-RES-8 mostrou ser uma medida unidimensional de empowerment em indivíduos com doença reumática com elevada consistência interna (alfa de Cronbach = 0.94). O empowerment mostrou estar positivamente relacionado com o nível percecionado de qualidade de vida. Em particular, os resultados revelaram associações positivas entre o empowerment, avaliado pelo PRES- 8, e cada um dos oito domínios do MOS SF-36. As associações foram de maior magnitude para a saúde mental e a perceção geral da saúde. Os resultados também revelaram que o empowerment se encontra positivamente associado com o nível de escolaridade dos doentes e com o número de anos após o diagnóstico. Os resultados forneceram suporte à adequação do P-RES-8 como medida de empowerment em pacientes com doença reumática, que revelou ser uma variável importante na avaliação da qualidade de vida dos pacientes.
Palavras-chave: Empowerment na doença crónica · Doenças reumáticas · Psicometria · Qualidade de vida · Psicologia da saúde
Introduction
Empowerment is a widely used concept in many disciplines. Empowerment is defined as “a process, a mechanism by which people, organizations, and communities gain mastery over their affairs” 1. One of the most fundamental dimensions of empowerment is self-efficacy which comprises the ideas of a sense of self-worth and believe in one’s capacities to manage and influence personal life situations ( 2 , 3 ). In fact, in health promotion, it is described as a process through which people get more control over decisions and actions that affect their health 4. For a successful chronic disease management, patients need to make choices in order to accomplish their personal and health-related goals 5. The empowerment approach highlights the importance of helping patients to think critically and make autonomous and informed decisions about their condition by self-management 6. Patients’ self-management implies being able to manage the symptoms, treatment, and physical and psychosocial consequences or lifestyle changes related to the chronic condition 7. An empowerment approach is particularly appropriate in diseases such as diabetes 6, but also in rheumatic diseases, which can have a significant impact on patients’ physical, mental, and social life ( 8 12 ). In rheumatology care, patient education is considered to be one way to reduce disability and to attain a better quality of life 13. Hence, the goal of education is to empower patients so that they can manage their lives and their symptoms and live as independently as they can 14.
In recent years, a range of measures have been developed to assess health-related empowerment ( 15 16 17 ). Based on an earlier work in diabetes education, Anderson et al. 18 developed the Diabetes Empowerment Scale (DES) in order to assess the psychosocial self-efficacy of patients with diabetes. The pilot version of the DES was a 37-item Likert-type questionnaire representing 8 conceptual dimensions: assessing the need for change, developing a plan, overcoming barriers, asking for support, supporting oneself, coping with emotion, motivating oneself, and making diabetes care choices appropriate for circumstances. This self-assessment questionnaire was then reduced to 28 items containing 3 subscales: (1) managing the psychosocial aspects of diabetes; (2) assessing dissatisfaction and readiness to change; and (3) setting and achieving diabetes goals 18. Later, an 8-item short form of the DES (DES-SF) was created to briefly assess patients’ self-efficacy 19. The authors chose the item with the highest item-to-subscale dimension correlation from each of the 8 original conceptual dimensions. This version demonstrated good evidence for reliability (α = 0.84) and validity 19. In 2013, the DES-SF was translated and adapted to Portuguese and then applied to a sample of diabetic patients 20. Cronbach’s α coefficient was found to be 0.87, and test-retest reliability ranged from 0.93 to 1.00.
Although created as an empowerment measure in diabetes care, the DES has been translated into different languages and used in patients with other chronic conditions (e.g., end-stage renal disease 21), including rheumatic diseases 22. A modified version of the DES-SF was created in Korea (Health Empowerment Scale – K-HES), replacing the term “diabetes” by “health problems” and expanding the items to cover all kinds of health conditions that affect the elderly 23. We did not find any study that has adapted the DES-SF to rheumatic patients.
Considering the lack of a Portuguese empowerment instrument for patients with rheumatic diseases, we developed the Portuguese Rheumatic Disease Empowerment Scale (P-RES-8), based on the already existing Portuguese version of the DES-SF. Therefore, this study aims to determine the psychometric qualities of the P-RES-8, such as reliability and validity. First, to analyze construct validity of the instrument, an exploratory factor analysis was conducted to assess the scale’s dimensionality. The internal consistency of the measure was analyzed in order to determine its reliability. Then, the associations between empowerment and self-perceived health status (Medical Outcomes Survey Short Form-36; MOS SF-36) were calculated to analyze the validity of the P-RES-8. Finally, the correlation between empowerment and other variables (education and illness duration) was examined to verify the criterion validity of the measure in patients with rheumatic disease.
Materials and Methods
Participants and Procedures
A total of 81 patients attending the Rheumatology Department at 2 public Portuguese hospitals were recruited for this cross-sectional study. Eligible patients included those diagnosed with a rheumatic disease, over 18 years old, able to understand and answer self-report questionnaires, and willing to participate in this study. The study protocol received the approval of both hospitals’ Ethics Committees, and written informed consent was obtained from patients who agreed to participate. All patients were diagnosed by a specialist and met the American College of Rheumatology criteria for classification of a rheumatic disease.
Measures
Written permission was obtained from the authors of the original and Portuguese versions of the DES-SF to adapt the instrument to rheumatic disease. The original scale was altered by changing the word “diabetes” to “rheumatic disease” in all items. The P-RES-8 is an 8-item Likert-type scale ranging from 1 (totally disagree) to 5 (totally agree), and it is scored by averaging the scores of all completed items. Higher scores suggest a greater level of perception of empowerment. According to previous research 22, we reasoned that self-efficacy and control over the disease should be positively related to perceived quality of life. So, to establish validity and test correlations between P-RES-8 scores and patients’ self-perceived health status, the Portuguese validated version of the MOS SF-36 24 questionnaire was used. This instrument measures the quality of life of the general population, and it is also applicable to patients with chronic diseases, since it evaluates the subjective perception concerning the impact of an underlying illness. Evidence has shown the MOS SF-36 to be a psychometrically valid measure to assess the quality of life in patients with rheumatic diseases ( 24 , 25 ). It includes 36 items covering the following 8 domains: physical functioning, physical performance, bodily pain, general health, social functioning, emotional well-being, mental health, and energy/fatigue. The scores obtained in each domain range from 0 to 100 with higher scores corresponding to higher levels of quality of life. Patients also filled in a questionnaire that included sociodemographic data and disease-related variables.
Statistics
All statistical analyses were calculated using SPSS software (IBM SPSS Statistics 23.0). To test the dimensionality of the P-RES-8, an exploratory factor analysis was conducted. Kolmogorov-Smirnov test results for each variable showed that normality of data was not assured ( p < 0.000). As a result, nonparametric correlation tests (Spearman rank order correlation) were used for all analyses. Statistical significance was considered as a p value of < 0.05.
Results
Patients had a mean age of 59.7 years (standard deviation (SD) 12.24), ranging from 31 to 79 years, and 77.8% were women ( n = 63). The majority were married or in a registered partnership (71.3%), 15% were widowed, and the remaining were either single or divorced. Most had less than 9 years of education (62%), and 16.5% had graduated. Nearly half of the participants were retired (44.4%), 27.2% were employed full time, and 14.8% were unemployed. Rheumatic diagnoses were combined into the following groups, as proposed by the American Rheumatism Association Nomenclature and Classification of Arthritis and Rheumatism (1983) 26: diffuse connective tissue diseases (50.6%), extraarticular disorders (24.7%, of which 22.2% were fibromyalgia), spondyloarthritis (11.1%), osteoarthritis (9.9%), neurovascular disorders (2.5%), and bone and cartilage disorders (1.2%). The mean illness duration of all patients was 8.67 years (SD 9.24).
Regarding the exploratory factor analysis results of the P-RES-8, the Kaiser-Mayer-Olkin index was 0.89, and Bartlett’s sphericity test was significant, χ 2 (28) = 499.64, p < 0.001, indicating the adequacy of the data for factor analytic procedures. The factorial free-extraction method was used, and a 1-factor solution was suggested by application of the Scree test criterion. The 8-item scale of the measure, which comprised only 1 factor (eigenvalue = 4.96), explained 62.04% of the total variance. Factor loadings and item communalities, after the exploratory factor analysis, are presented in Table 1 .
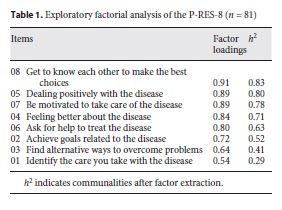
All the factor loadings obtained are higher than 0.50, and the communalities are also satisfactory for all the 8 items of the scale. Internal consistency was high (Cronbach’s α = 0.94). Cronbach’s α values, if the item was deleted, varied between 0.91 (item 08) and 0.93 (item 01). All inter-item correlations were significant ( p < 0.001) and varied between 0.36 and 0.83. The frequencies and descriptive statistics (mean, SD, skewness, and kurtosis) of the responses to each of the items of the P-RES-8 are presented in Table 2 . The results show an acceptable variability of response distribution to the scale items.
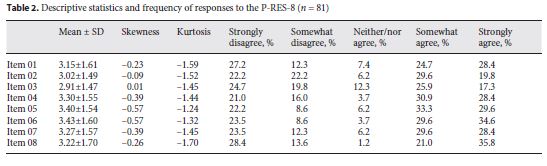
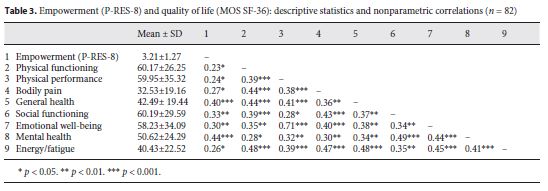
Table 3 exhibits the means, SDs, and intercorrelation matrix for empowerment and MOS SF-36 dimensions. The mean scores of the MOS SF-36 are below 65% for all domains of this instrument. Therefore, the quality of life assessed by the MOS SF-36 is revealed to be relatively low, in particular in the bodily pain domain (mean 32.63). The empowerment measure P-RES-8 is positively and significantly related to all the domains of quality of life, and all the correlations are above 0.25. Particularly, the associations are stronger for mental health ( r - s = 0.44, p < 0.001) and general health perception ( r - s = 0.40, p < 0.001). Considering the correlations between MOS SF-36 dimensions, the results show weak to moderate, significant and positive associations between all variables, as expected by the authors of the Portuguese version of the instrument 27. Moreover, significant positive associations were also obtained between empowerment and component summary scores of mental ( r - s = 0.36, p = 0.001) and physical functioning ( r - s = 0.23, p = 0.043). Finally, associations between empowerment and individual variables (patients’ education and years after diagnosis) were analyzed. Results showed that empowerment is positively associated with years of education ( r - s = 0.29, p = 0.009) and years after diagnosis ( r - s = 0.29, p = 0.009).
Discussion
The main purpose of this study was to provide support for the psychometric qualities of an empowerment measure for patients with rheumatic diseases. Participants in this study were mostly women, middle-aged, married, and with a low level of education. The obtained results showed relatively low scores for all the domains of the MOS SF-36, and pain was considered the most important domain limiting quality of life, as suggested by previous research 28.
The construct validity of the P-RES-8 was confirmed because the 1-factor structure of the P-RES-8 scale was obtained, in accordance with previous studies using this health-related empowerment measure ( 19 , 20 , 23 ). Moreover, internal consistency of the instrument was high. The criterion validity of the P-RES-8 was supported by the direction and significance of the associations found between patient empowerment and quality of life, also described in other studies with patients with rheumatic disease 22. In fact, empowerment was positively associated with all dimensions of patients’ quality of life, which means that, as the sense of control in disease management increases, so does patients’ perception of their quality of life. Particularly, patients’ empowerment was moderately associated with the domains of mental health and general health. This result highlights the importance of patients’ perception of their own power and control over the disease in the appraisal of general health and psychological state.
Additional evidence for the validity of the P-RES-8 is sustained by the correlations between empowerment and other relevant variables. Specifically, higher levels of empowerment were reported by patients with a higher education, which was also found in the study by Anderson et al. 18 on patients with diabetes. Moreover, empowerment levels were positively correlated with the duration of the disease. This finding may be explained by the increasing use of more adaptive illness-related coping strategies over time, which contributes to a perception of greater control over the disease.
This study has some limitations that should be taken into consideration when interpreting the results. First, this is a cross-sectional and correlational study which allows us to draw conclusions from the associations between variables but not concerning cause-effect relations. Also, the representativeness of the sample can be questioned due to its size, type (convenience sample), recruitment hospitals, and demographic characteristics (e.g., gender, age, and education). Finally, the sample comprises several rheumatic diagnoses with different symptoms and impacts on patients’ quality of life. Nonetheless, to minimize the disadvantages of using small samples in scale development, we intended to maximize the sample size, particularly to ensure the variance of data conditions 29. Further studies with other groups of rheumatic diseases, including 1-disease samples, are required to confirm the factor structure and reliability of the scale. Also, future studies should consider analyzing test-retest reliability to assess how constant scores remain from one occasion to another 29. Despite these limitations, as previously stated, the main purpose of this research was to study the psychometric qualities of the P-RES-8, and the results are adequate to conclude on the validity and fidelity of this measure. Furthermore, the results obtained are consistent with other empirical findings reinforcing the validity of the P-RES-8 scale in assessing the sense of empowerment in rheumatic patients.
Conclusion
Empowerment is recognized as a significant outcome of effective health-care interventions in chronic disease ( 17 , 30 , 31 ) as well as an important indicator of patients’ self-management and adjustment to disease. This study provides preliminary support for the validity and reliability of the P-RES-8 as a measure of perception of empowerment in patients with rheumatic diseases. Further studies are needed to ensure that the instrument is appropriate to assess the efficacy of health education programs.
REFERENCES
1 Rappaport J: Terms of empowerment/exemplars of prevention: toward a theory for community psychology. Am J Community Psychol 1987; 15: 121–148. p. 122.
2 Rogers ES, Chamberlin J, Ellison ML, Crean T: A consumer-constructed scale to measure empowerment among users of mental health services. Psychiatr Serv 1997; 48: 1042–1047.
3 Rogers ES, Ralph RO, Salzer MS: Validating the empowerment scale with a multisite sample of consumers of mental health services. Psychiatr Serv 2010; 61: 933–936.
4 WHO: Health Promotion Glossary. Geneva, World Health Organization, 1998. http://www.who.int/healthpromotion/about/HPR%20Glossary%201998.pdf (accessed July 26, 2016). [ Links ]
5 Feste C, Anderson RM: Empowerment: from philosophy to practice. Patient Educ Couns 1995; 26: 139–144.
6 Anderson RM, Funnell MM: Patient empowerment: myths and misconceptions. Patient Educ Couns 2010; 79: 277–282.
7 Barlow J, Wright C, Sheasby J, Turner A, Hainsworth J: Self-management approaches for people with chronic conditions: a review. Patient Educ Couns 2002; 48: 177–187.
8 Gettings L: Psychological well-being in rheumatoid arthritis: a review of the literature. Musculoskeletal Care 2010; 8: 99–106.
9 Anyfanti P, Gavriilaki E, Pyrpasopoulou A, Triantafyllou G, Triantafyllou A, Chatzimichailidou S, et al: Depression, anxiety, and quality of life in a large cohort of patients with rheumatic diseases: common, yet undertreated. Clin Rheumatol 2016; 35: 733–739.
10 Duarte C, Abreu P, Couto M, Vaz C, Malcata A, Inês L: Health related quality of life in Portuguese SLE patients: an outcome measure independent of disease activity and cumulative damage. Acta Reumatol Port 2010; 35: 30–35.
11 Kool MB, Geenen R: Loneliness in patients with rheumatic diseases: the significance of invalidation and lack of social support. J Psychol 2012; 146: 229–241.
12 Lessinck ML, Burdorf A, Boonen A, Gignac MA, Hazes JM, Luime JJ: Consequences of inflammatory arthritis for workplace productivity loss and sick leave: a systematic review. Ann Rheum Dis 2013; 72: 493–505.
13 Ramos-Remus C, Salcedo-Rocha AL, Prieto RE, Galvan-Villegas F: How important is patient education? Best Pract Res Clin Rheumatol 2000; 14: 689–703.
14 Hill J: An overview of education for patients with rheumatic diseases. Nurs Times 2003; 99: 26–27.
15 Barr PJ, Scholl I, Bravo P, Faber MJ, Elwyn G, McAllister M: Assessment of patient empowerment: a systematic review of measures. PLoS One 2015; 10:e0126553. [ Links ]
16 Herbert RJ, Gagnon AJ, Rennick JE, O’Loughlin JL: A systematic review of questionnaires measuring health-related empowerment. Res Theory Nurs Pract 2009; 23: 107–132.
17 McAllister M, Dunn G, Payne K, Davies L, Todd C: Patient empowerment: the need to consider it as a measurable patient-reported outcome for chronic conditions. BMC Health Serv Res 2012; 12: 157. [ Links ]
18 Anderson RM, Funnell MM, Fitzgerald JT, Marrero DG: The Diabetes Empowerment Scale: a measure of psychosocial self-efficacy. Diabetes Care 2000; 23: 739–743.
19 Anderson RM, Fitzgerald JT, Gruppen LD, Funnel MM, Oh MS: The Diabetes Empowerment Scale-Short Form (DES-SF). Diabetes Care 2003; 26: 1641–1642.
20 Aveiro M, Santiago LM, Ferreira PL, Simões JA: Fiability study of Diabetes Empowerment Scale: short version (in Portuguese). Acta Med Port 2015; 28: 177–181.
21 Tsay SL, Hung LO: Empowerment of patients with end-stage renal disease: a randomized controlled trial. Int J Nurs Stud 2004; 41: 59–65.
22 Arvidsson S, Bergman S, Arvidsson B, Fridlund B, Tingsröm P: Psychometric properties of the Swedish Rheumatic Disease Empowerment Scale, SWE-RES-23. Musculoskeletal Care 2012; 10: 101–109.
23 Park C, Park YH: Validity and reliability of Korean version of health empowerment scale (K-HES) for older adults. Asian Nurs Res 2013; 7: 142–148.
24 Baba S, Katsumata Y, Okamoto Y, Kawaguchi Y, Hanaoka M, Kawasumi H, et al: Reliability of the SF-36 in Japanese patients with systemic lupus erythematosus and its associations with disease activity and damage: a two-consecutive year prospective study. Lupus 2018; 27: 407–416.
25 Klooster PM, Vonkema HE, Taal E, Siemons L, Hendriks L, Jong AJ, et al: Performance of the Dutch SF-36 version 2 as a measure of health-related quality of life in patients with rheumatoid arthritis. Health Qual Life Outcomes 2013; 11: 77. [ Links ]
26 Decker JL: American Rheumatism Association nomenclature and classification of arthritis and rheumatism (1983). Arthritis Rheum 1983; 26: 1029–1032.
27 Ferreira PL: Development of the Portuguese version of MOS SF-36. Part I. Cultural and linguistic adaptation. Acta Med Port 2000; 13: 55–66.
28 Leino-Kilpi H, Maenpaa I, Katajisto J: Nursing study of the significance of rheumatoid arthritis as perceived by patients using the concept of empowerment. J Orthop Nurs 1999; 3: 138–145.
29 DeVellis FR: Scale Development: Theory and Applications, ed 4. Thousand Oaks, Sage, 2016. [ Links ]
30 Evers AW, Zautra A, Thieme K: Stress and resilience in rheumatic diseases: a review and glimpse into the future. Nat Rev Rheumatol 2011; 7: 409–415.
31 Anderson RM, Funnel MM, Butler PM, Arnold MS, Fitzgerald JT, Feste CC: Patient empowerment: results of a randomized controlled trial. Diabetes Care 1995; 18: 943–949.algorithms.
Received: January 24, 2018. Accepted: June 5, 2018

