










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Public Health
versão impressa ISSN 2504-3137versão On-line ISSN 2504-3145
Port J Public Health vol.38 no.1 Lisboa 2020
https://doi.org/10.1159/000508634
RESEARCH ARTICLE
Spatiotemporal Analysis of Breast Cancer Hospitalizations in Portugal in 2002–2016
Análise espácio-temporal de hospitalizações por cancro da mama em Portugal em 2002–2016
Inês Afonso Gomes a c Bruno Moita a, d Carla Nunes a, c
a Escola Nacional de Saúde Pública, Universidade Nova de Lisboa, Lisboa, Portugal;
b Pfizer, Porto Salvo, Portugal;
c Centro de Investigação em Saúde Pública (CISP), Universidade Nova de Lisboa, Lisboa, Portugal;
d Centro Hospitalar Universitário do Algarve, Faro, Portugal
ABSTRACT
Introduction: Breast cancer (BC) is the most common cancer among Portuguese women and it is associated with high hospitalization rates. Therefore, this study aims to characterize the BC hospital admission rate (HAR) in women in the period of 2002–2016, with an additional focus on spatiotemporal patterns of hospitalizations by BC (main code). - Methods: After a descriptive analysis of all BC hospitalizations, the main BC code HAR was studied using mapping techniques, analysis of spatiotemporal clusters, and analysis of spatial variations in temporal trends. - Results: The BC-HAR was 118.72/105 women, showing a growth of 3.109% per year in this period. The median length of stay (LOS) in these patients was 5 days, and most cases were programmed surgical admissions. Several spatiotemporal clusters and spatial variations in temporal trends were detected. The seaside area of the country showed 4 high HAR clusters in the spatiotemporal analysis. Additionally, the seaside north of the country and 2 isolated counties presented significantly different temporal trends in BC-HAR versus the rest of the country. These clusters suggest regional asymmetries, as they showed differences in terms of: demographic characteristics (age at admission and rurality of county of residence), the type of admission, LOS, and outcomes of hospitalization. - Conclusion: This study identified key areas of high BC-HAR and increasing trends for female HAR, providing evidence of spatial heterogeneities in this health indicator.
Keywords: Breast neoplasms; Spatiotemporal analysi; Hospitalization; Portugal
RESUMO
Introdução: O cancro da mama é a neoplasia mais comum em mulheres Portuguesas e é responsável por elevadas taxas de hospitalização. Como tal, este estudo pretende caracterizar as admissões hospitalares por cancro da mama feminino no período de 2002–2016, com foco adicional nos padrões espácio-temporais das hospitalizações por cancro da mama (código principal). Métodos: Após uma análise descritiva de todas as hospitalizações com código de cancro da mama, os internamentos com código principal para esta patologia foram estudados com recurso a técnicas de mapeamento, análise de clusters espácio-temporais e variações espaciais em tendências temporais. Resultados: A taxa de internamento hospitalar por cancro da mama foi 118.72/105 mulheres, mostrando um crescimento de 3.109%/ano neste período. A mediana do tempo de hospitalização nestas doentes foi 5 dias, e a maioria dos internamentos corresponderam a admissões cirúrgicas programadas. Vários clusters espácio-temporais e variações espaciais em tendências temporais foram detetados. A zona costeira do país apresentou 4 clusters com elevada taxa de internamento hospitalar na análise espácio-temporal. Adicionalmente, a zona norte costeira e 2 concelhos isolados exibiram tendências temporais significativamente diferentes das descritas no resto do país. Estes clusters sugerem assimetrias regionais, apresentando divergências nas características demográficas (idade de admissão e ruralidade do concelho de residência), tipo de admissão, tempo de internamento e outcome da hospitalização. Conclusão: Este estudo identificou áreas chave de elevada taxa de internamento hospitalar por cancro da mama e uma tendência crescente nestes internamentos, fornecendo dados sobre a heterogeneidade espacial neste indicador de saúde.
Palavras Chave: Cancro da mama · Análise espácio-temporal · Hospitalização · Portugal
Introduction
Breast cancer (BC) is the most frequent malignant disease in women and it represents a large disease burden, being a major cause of cancer-associated hospital discharges in European women and numerous hospital admissions [1 - 5 ]. Several studies have indicated that the majority of hospital admissions in BC patients are due to major surgeries and that the number of hospitalizations in these patients are associated with the presence of comorbidities and the stage of the disease [6 - 12 ]. Furthermore, a study conducted in 2002–2004 in Spain showed a differential BC hospital admission rate (HAR) in different areas due to older age and local variation in BC incidence 5.
The median hospital length of stay (LOS) in BC patients varies according to the studies considered, ranging from 1.7 to 14.5 days [5 ,6 ,8 ,12 - 17 ]. Additionally, the LOS of BC patients has been associated with the stage at diagnosis, the presence of comorbidities, deprivation, age, surgical procedure,and year of analysis (6 and 5 days in 1996 and 2006, respectively, and 5 and 4 days in 1997/1998 and 2004/2005, respectively) [14 ,15 ,17 - 21 ].
The published literature indicates that the BC-associated hospital production and the number of surgeries for BC management have been increasing in the last decade in Portugal [3 ,22 - 24 ] (online suppl. table 1, 2; see www.karger.com/doi/10.1159/000508634 for all online suppl. material). Another publication pointed that, in the period of 2000 to 2008, BC was responsible for 9.5–9.7% of hospitalizations and 3.6–5.6% of deaths during hospitalization in cancer patients 24. The majority of hospitalizations in BC patients described in this study were women aged 45–64 years, and regional asymmetries were reported both in hospitalization and in-patient deaths 24.
The monitoring of hospitalizations, i.e., regional differences and trend variations, can provide powerful insights for the assessment/setting of public health policies, estimation of the burden and status of health conditions, and planning of resource allocation [4 ,25 - 27 ]. Differences in hospital procedures, treatment patterns, and outpatient resources might lead to regional differences in hospitalization lengths among different areas 14. The analysis of discharged BC patients can also be a useful tool for monitoring the burden of the disease/patterns at national and local levels 26.
Therefore, the main goal of this study was to describe the female hospitalizations related to BC (both main and secondary causes of admission) and conduct a spatiotemporal analysis of main BC admission hospitalizations between 2002 and 2016 in Portugal. Additionally, a characterization of the spatiotemporal patterns of female BC hospitalizations and assessment of the differences in the clusters identified were conducted in this study.
Methods
Data and Sources
The hospital admissions of female patients with BC (codes 174.0–174.9 of the ICD 9) in 2002–2016 were obtained from the hospital morbidity database (BDMH). After exclusion of same-day admissions, both patients with main ( n = 100,148) and secondary ( n = 36,459) BC admission codes (up to a maximum of 20 diagnosis codes) were included in this study in order to have complete assessment of the burden of this disease in hospital production [5 - 9 ,12 - 16 ,24 - 31 ]. This database, containing all of the admissions occurring in national healthcare service (SNS) Portuguese mainland hospitals, was obtained from the Administração Central do Sistema de Saúde (ACSS) and had been previously anonymized.
The median female population per county/year and the median population density was calculated from data freely available at Statistics Portugal 32.
Methods
Firstly, a descriptive analysis of BC hospital admissions was done for patients with main and secondary BC admission information (i.e., year of admission, LOS, destination after discharge, type of admission, age at admission, rurality of residence county, and main admission code). Patients were divided into the following 4 age groups based on the literature: <40, 40–49, 50–64, and ≥65 years [2 ,33 - 43 ]. Patients aged ≥100 years ( n = 21; 0.012%) were excluded from the analysis, as were patients with an LOS of 0 days ( n = 44,779; 25.8%).
The median population density in the period of analysis was calculated for each of the counties, and cut-off values of 150 and 300 inhabitants/km 2 were applied for the definition of rural, intermediate, and urban areas 44. The annual HAR was defined as the number of female hospitalizations with a BC admission code in a certain area in a determined year, divided by the median population (at June 30) of female inhabitants in that same area and year 45. The HAR for the main and secondary and all BC admission codes were determined (as crude rates) per year and globally (entire period). The HAR was expressed per 10 5 inhabitants. Additionally, for patients with a main BC admission code, temporal and spatiotemporal clusters plus the detection of spatial variations in temporal trends were identified [6 ,8 ,9 ,12 - 14 ,16 ,24 ,26 ,28 - 30 ]. Patients without a valid residence county code ( n = 7,536; 7.5%) or resident in the insular Madeira and Açores areas ( n = 147; 1.5%) were not included in this analysis. This analysis was conducted using SaTScan TM software (version 9.4.4; Martin Kulldorff, Boston, MA, USA), applying circular windows with a maximum of 20% of the studied population and using a discrete Poisson model. The spatial unit used in the spatiotemporal analysis was the mainland counties ( n = 278). The significance level was set at 0.05. The comparison between spatial variations in temporal trend clusters was done using a nonparametric test of median comparisons and the χ 2 test for independency (for the remaining comparisons). Descriptive analysis and statistical tests comparing the characteristics of the clusters identified were conducted in Statistical Package for Social Sciences (SPSS TM,version 22 for Windows; IBM Corp., Armonk, NY, USA), and the results were mapped using QGIS TM software (version 2.18s; Free Software Foundation Inc., Boston, MA, USA).
Results
Country Analysis
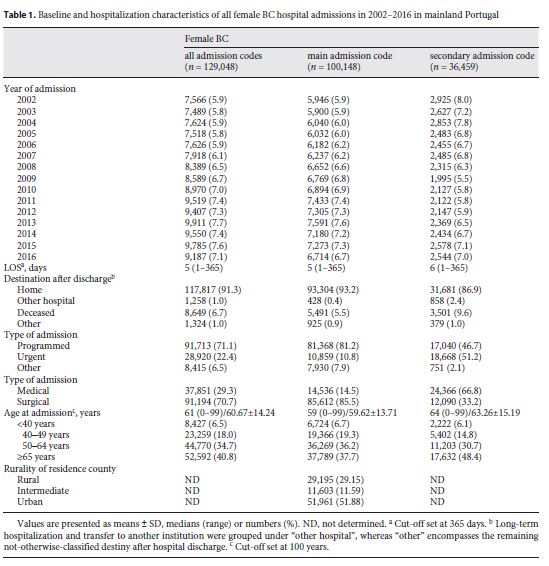
In the period between 2002 and 2016, for patients with a main BC admission code the malignant neoplasm of other specified sites of the female breast (41.9%) or of the upper-outer quadrant of the female breast (29.0%) were the most common code of admission. Admissions for radiotherapy (4.1%), chemotherapy/immunotherapy (3.8%), fitting and adjustment of vascular catheter (2.4%), (drug-induced) neutropenia (6.5%), secondary malignant neoplasms (8.8%), pneumonia (3.7%), congestive heart failure (1.5%), and urinary tract infection (1.5%) represented the main admission codes for patients with secondary BC codes. Additionally, 19.2% of the patients with a secondary BC code had a main BC code at admission (15.5%). Demographic characteristics of the patients with BC admission codes can be found in table 1 .
Although the median LOS of patients with BC as the main admission code was similar to that shown for all hospitalizations with BC admission codes, the median age at admission was lower in the first group (5 days and 59 years, respectively). Most (85.5%) of these patients were admitted for surgical procedures, versus 33.2% for patients with secondary BC admission codes. Furthermore, patients with secondary BC admission codes showed a higher LOS than those with a main BC admission code (6 days). Additionally, a higher percentage of patients with secondary BC admission codes were admitted as urgent (51.2 vs. 10.8% for a main BC admission code).
Analysis by County (n = 278)
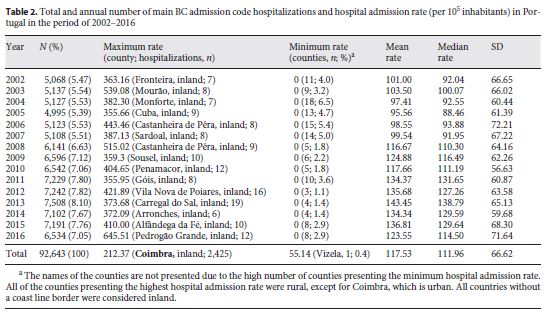
The Portuguese counties presenting the highest HAR for patients with a main BC admission code varied over time. In each of the analyzed years, 1.1–6.5% of the counties showed no hospitalizations with a main BC admission code; however, no counties presented no hospitalizations with this cancer code in the period of 2002–2016 (table 2 ).
Spatiotemporal Analysis by Counties (n = 278)
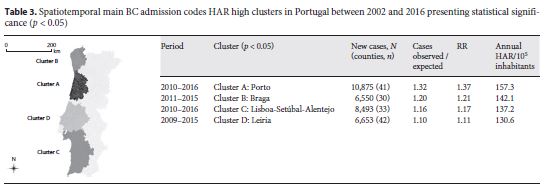
In the period of 2002–2016 ( n = 92,643), the annual female HAR for BC main admission codes was 118.72/10 5 inhabitants, showing a growth of 3.109% per year. Additionally, the period of 2009–2015 showed a significantly higher HAR than the remaining analyzed years (135.2/10 5 inhabitants, relative risk [RR] = 1.39; p = 0.001). Several statistically significant high HAR spatiotemporal clusters for main BC admission codes were identified and are described in table 3 . Additionally, details on the spatial variations in temporal trends clusters identified in mainland Portugal are further described below in table 4 and figure 1 .
Discussion/Conclusion
To our knowledge, this study is the first spatiotemporal analysis conducted on the hospitalization of BC patients, providing a basis for future studies using this methodology and further analysis on the BC burden among Portuguese women.
Most counties showed cases of BC hospitalizations in the period of 2002–2016, and most of these hospital admissions (77.61%) presented BC as the main admission code. The median age at admission of patients with BC admission codes was 61 years, which is slightly higher than prior data published for Portuguese patients in 2008 (median age: 59 years) 24. The median LOS observed in this period was 5 days, which falls within the range published for BC patients, showing a decrease from 7 days in 2002 to <4 days from 2010 onwards (data not shown); this is in agreement with previously reported data [5 ,6 ,8 ,12 - 16 ,18 ,46 ]. This decrease in LOS could be a result of diagnosis at earlier stages or the evolution of surgical procedures over time [14 ,18 ,19 ]. A total of 71.1% of the analyzed hospitalizations were programmed, and 70.7% of admissions corresponded to surgical interventions, matching the published data [6 - 9 ]. Additionally, 91.3% of the patients were discharged to their homes, whereas 6.7% died during their hospital admission; this represents a higher hospital lethality than that previously published on Portuguese BC patients (3.6–5.6%) 24, and this fact could potentially be explained by the inclusion of both main and secondary BC diagnosis in the present study.
The main BC admission code HAR in mainland Portugal was 118.72/10 5 inhabitants, which is in the range of previously reported rates (111.1–140.5/10 5 inhabitants) 47, whereas the HAR for secondary and all BC codes were 42.36 and 153.34/10 5 inhabitants (0.91 admissions/h). The HAR for all BC admissions showed an increase over the studied period, i.e., from 125.73/10 5 inhabitants in 2002 (0.74 admissions/h) to 173.10/10 5 inhabitants (1.02 admissions/h) in 2016; this trend is similar to that reported for Spain 47.
The increase in BC admission codes was mostly noticed in the last (2009–2016) versus the earlier years of the analysis (2002–2008) and could reflect changes in the hospital billing mindset, the outcome of coding training sessions, sub-notification of this disease in the beginning of the period of analysis, an increase in the incidence of this cancer in the Portuguese population, or improved survival among these patients [3 ,22 ,23 ,48 - 50 ]. Additionally, some heterogeneous coding patterns were detected throughout the country in terms of all and secondary admission codes. These regional asymmetries should be further evaluated to determine local needs for further health investment or the need for changes in BC patients’ follow-up plan.
The mainland main BC code HAR showed a flat period from 2002 to 2007, increasing from 117.51/10 5 inhabitants in 2008 to 126.34/10 5 inhabitants in 2016 (the maximum HAR in 2013 reached: 143.97/10 5 inhabitants) (online suppl. table 3). Additionally, the temporal variation in hospitalizations of patients with main BC admission codes was +3.109%/year, which is similar to the growth of incidence reported in a previous study conducted in the south of Portugal (+4.113%/year) 48. This parallelism could point to a link between BC incidence and hospitalizations with BC as a main admission code or a good referral of newly diagnosed cases to surgical treatment (which corresponded to 85.5% of the cases with a main BC admission code), a link that could potentially be explored to complement cancer registries data. This growth in BC-HAR is concordant with the published data on this topic [3 ,22 - 24 ] and could reflect an increased incidence and prevalence of BC in this population, highlighting the need to prepare healthcare systems to handle the higher demand by cancer patients, or the presence of incomplete data in the database on the earlier years of the studied period due to limitations in the coding field.
Most of the counties identified as presenting the highest HAR in each of the analyzed years corresponded to small rural populations with a low number of inhabitants (small numbers). The only exception detected (Coimbra for 2002–2016) could potentially be explained by the referral of patients to the specialized oncology center in Coimbra; however, further analyses are of paramount relevance to detect any overuse of hospital services by BC patients in these areas or identify the reasons for the higher prevalence of BC in this county.
The spatiotemporal clusters identified for main BC admission codes, located in the northwest (clusters A and B) and southwest coasts of the country (clusters C and D), showed an RR ranging from 1.37 to 1.11, with the highest RR being reported in the north of the country. The 2 southern clusters (clusters C and D) align geographically and temporally with previously published data on areas with a high BC incidence in 2009 22, further supporting the link between incidence and HAR in BC patients.
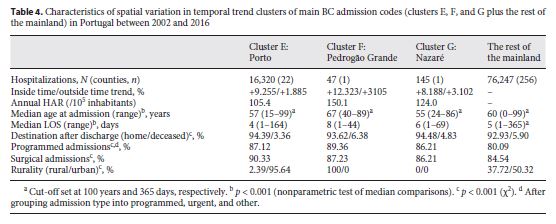
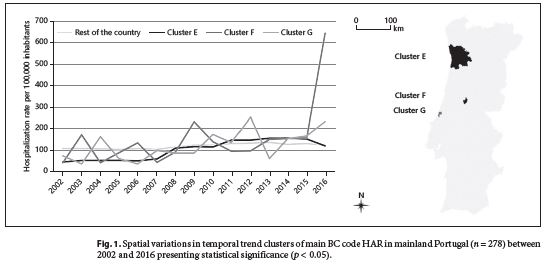
The spatial variations in the temporal trend analysis of main BC admission code hospitalizations identified 3 clusters for which the behavior of HAR over time was statistically different from the country trend (table 4 ). Whereas the HAR in the rest of the country slowly increased over the studied period (∼170–180/10 5 inhabitants), the HAR in cluster E doubled in 2008, growing then more slowly toward the national trend. On the other hand, clusters F and G showed high variations in BC-HAR over the studied period (Fig. 1 ). The differential behavior of these regions could have to do with coding variances in the hospitals of different regions, population differences in terms of BC incidence/prevalence, or differential needs for care of the populations of these regions.
When looking into the 3 clusters identified in the spatial variations in temporal trend analysis of the main BC admission codes, cluster F presented a higher median age at admission than the rest of the mainland, whereas clusters E and G shower a significantly lower median age at admission. This discrepancy in the age at admission could be the result of an older resident population in the cluster F county (≤64 years: 83, 79, and 63% in clusters E, G, and F, respectively). The LOS was significantly different between these 3 clusters and the rest of the country, with clusters F and G showing the highest median (8 and 6 days, respectively). Cluster E presented the highest relative number of surgical admissions, which could potentially be explained by the hospitalization of more newly diagnosed BC cases at the oncologic center located in that area. Cluster F showed the highest lethality rate among BC admissions (6.38%), and cluster E and the rest of the country showed concordant results on this outcome for the respective geographic areas (3.4–6.5 and 5.2–8.7%, respectively) 24. This increased lethality can be a result of numerous factors such as the older population or the rural nature of the county, which could potentially decrease healthcare access and lead to a later diagnosis of these patients. The 3 clusters also showed divergences in their baseline demographics, with most patients in cluster E being from urban areas, whereas the ones in cluster F were from a rural setting. These differences are outside of the scope of this study but could eventually impact the patient’s outcome during hospitalizations or even point to the potential cancer care organizational differences in the different areas of the country. Therefore, further studies are needed to assess these regional asymmetries, i.e., in terms of the characteristics of the hospitalization (admission for cancer therapies such as radiation or chemotherapy, number of comorbidities, or presence of complications).
The spatiotemporal and the spatial variation in temporal trend clusters also showed some similarities, with clusters A and E almost perfectly overlapping geographically. These resemblances point to a disparity in the behavior of BC hospitalizations in these areas, translated into temporal trends that are statistically different from the national trend, and reinforce the complementary of these statistical methods in the detection of spatial and temporal critic areas/periods. Further studies should be carried out to clarify these findings and to assess whether the growing BC-HAR trends persisted after the studied period, especially considering that the high BC-HAR spatiotemporal clusters were detected in the later years of the analysis. Additionally, the BC incidence and mortality rate should be analyzed together with the HAR in this population to get a more accurate picture of the reality of this malignancy in Portugal.
This study has some limitations, such as the impossibility of determining repeated admissions of the same patient over the studied period, the changes in the geographic boundaries of regions (different geographical administrative organization) during the analyzed years, and the possibility of incomplete information or coding errors in some registries. Additionally, as coding of admissions is conducted at a local level, some regional differences could be the result of local coding guidance. Moreover, the occurrence of training coding sessions could have influenced the spatial and temporal distribution of BC hospitalizations in this period; therefore, the differences identified could result in increased notification rather than an actual growth of HAR among these patients. The increase in the number of diagnosis fields per hospitalization in 2011 and the growing focus on hospital costs could also have led to a more complete record of admission codes over time (hence the focus on the main admission codes in the present study).
Portuguese women have shown a growing BC-HAR; however, the trend for this increase varied according to the area of residence and the definition of BC hospital admission as a main or secondary admission code. The reasoning behind these different patterns could be related to the distribution of BC cases in the country, regional BC management guidelines, or the lack of health structures in some areas that can follow-up these patients outside of the hospital context [22 ,48 ]. Altogether, these data support the uneven distribution of BC hospitalizations reported previously in different Portuguese regions 24 and the need for further studies on this topic to evaluate potential inequalities in BC care.
REFERENCES
1 International Agency for Research on Cancer, World Health Organization. GLOBOCAN 2012: estimated cancer incidence, mortality and prevalence worldwide in 2012. 2020 (cited 2016 May 28). Available from: http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx. [ Links ]
2 Bray F, McCarron P, Parkin DM. The changing global patterns of female breast cancer incidence and mortality. Breast Cancer Res. 2004; 6(6): 229–39.
3 Ministério da Saúde, Direção-Geral da Saúde. Portugal: doenças oncológicas em números 2014: Programa Nacional para as Doenças Oncológicas. 2014 (cited 2019 Mar 17). Available from: https://www.dgs.pt/estatisticasde-saude/estatisticas-de-saude/publicacoes/portugal-doencas-oncologicas-em-numeros-2014-pdf.aspx. [ Links ]
4 Eurostat. Eurostat regional yearbook. Brussels: European Commission; 2011. pp. 69–78.
5 López-Jurado CF, Martínez-Sánchez JM, Anes Del Amo Y, Ramos-Aceitero JM. Mortalidad y frecuencia hospitalaria de tumor maligno de mama en Extremadura (2002–2004). Enferm Clin. 2008 Nov-Dec; 18(6): 296–301.
6 Iezzoni LI, Henderson MG, Bergman A, Drews RE. Purpose of admission and resource use during cancer hospitalizations. Health Care Financ Rev. 1991; 13(2): 29–40.
7 Hassett MJ, O’Malley AJ, Pakes JR, Newhouse JP, Earle CC. Frequency and cost of chemotherapy- related serious adverse effects in a population sample of women with breast cancer. J Natl Cancer Inst. 2006 Aug; 98(16): 1108–17.
8 Russo CA, Milenkovic M, Steiner C. Hospital stays for breast cancer, 2004: Statistical Brief #15. In: Russo CA, Milenkovic M, Steiner C, editors. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Rockville (MD): Agency for Healthcare Research and Quality; 2006. [ Links ]
9 Neutel CI, Gao RN, Wai E, Gaudette LA. Trends in in-patient hospital utilization and surgical procedures for breast, prostate, lung and colorectal cancers in Canada. Cancer Causes Control. 2005 Dec; 16(10): 1261–70.
10 Du XL, Osborne C, Goodwin JS. Populationbased assessment of hospitalizations for toxicity from chemotherapy in older women with breast cancer. J Clin Oncol. 2002 Dec; 20(24): 4636–42.
11 Enright K, Grunfeld E, Yun L, Moineddin R, Ghannam M, Dent S, et al. Population-based assessment of emergency room visits and hospitalizations among women receiving adjuvant chemotherapy for early breast cancer. J Oncol Pract. 2015 Mar; 11(2): 126–32.
12 Vin-Raviv N, Akinyemiju TF, Galea S, Bovbjerg DH. Depression and anxiety disorders among hospitalized women with breast cancer. PLoS One. 2015 Jun; 10(6):e0129169. [ Links ]
13 Tan SS, Hakkaart-van Roijen L, van Ineveld BM, Redekop WK. Explaining length of stay variation of episodes of care in the Netherlands. Eur J Health Econ. 2013 Dec; 14(6): 919–27.
14 Neutel CI, Gao RN, Gaudette L, Johansen H. Shorter hospital stays for breast cancer. Health Rep. 2004 Oct; 16(1): 19–31.
15 Day FL, Bull JM, Lombard JM, Stewart JF. Changes in medical oncology admissions for the management of breast cancer complications: an Australian institution’s experience. Asia Pac J Clin Oncol. 2011 Jun; 7(2): 146–53.
16 Ogunsina K, Naik G, Vin-Raviv N, Akinyemiju TF. Sequential matched analysis of racial disparities in breast cancer hospitalization outcomes among African American and White patients. Cancer Epidemiol. 2017 Aug; 49: 138–43.
17 Chang HT, Shi HY, Wang BW, Yeh SJ. Breast Cancer Incidence and Predictors of Surgical Outcome: a Nationwide Longitudinal Study in Taiwan. Clin Oncol (R Coll Radiol). 2017 Jun; 29(6): 362–9.
18 Downing A, Lansdown M, West RM, Thomas JD, Lawrence G, Forman D. Changes in and predictors of length of stay in hospital after surgery for breast cancer between 1997/98 and 2004/05 in two regions of England: a population- based study. BMC Health Serv Res. 2009 Nov; 9(1): 202. [ Links ]
19 Lindqvist R, Alvegard TA, Jönsson PE, Stenbeck M. Hospital stay related to TNM-stage and the surgical procedure in primary breast cancer. Acta Oncol. 2004; 43(6): 545–50.
20 Marla S, McMillan DC, Stallard S. Factors influencing postoperative length of hospital stay after breast cancer surgery. Breast. 2013 Jun; 22(3): 289–94.
21 Sun SX, Leung AN, Dillon PW, Hollenbeak CS. Length of stay and readmissions in mastectomy patients. Breast J. 2015 Sep-Oct; 21(5): 526–32.
22 Ministério da Saúde, Direção-Geral da Saúde. Portugal: doenças oncológicas em números 2015: Programa Nacional para as Doenças Oncológicas. 2016 (cited 2019 Mar 30). Available from: https://www.dgs.pt/estatisticasde-saude/estatisticas-de-saude/publicacoes/portugal-doencas-oncologicas-em-numeros-2015-pdf.aspx. [ Links ]
23 Ministério da Saúde, Direcção-Geral da Saúde. Portugal: doenças oncológicas em números 2013: Programa Nacional para as Doenças Oncológicas. 2013 (cited 2019 Apr 17). Available from: https://www.dgs.pt/estatisticas-de-saude/estatisticas-de-saude/publicacoes/portugal-doencas-oncologicas-emnumeros-2013-pdf.aspx. [ Links ]
24 Machado MC, Couceiro L, Alves I, Almendra R, Cortes M. A morte hospitalar. In: Alves I, Machado MC, Cortes M, Almendra R, Couceiro L, editors. A morte e o morrer em Portugal. Coimbra: Edições Almedina; 2011. [ Links ]
25 Trombert Paviot B, Gomez F, Olive F, Polazzi S, Remontet L, Bossard N, et al. Identifying prevalent cases of breast cancer in the French case-mix databases. Methods Inf Med. 2011; 50(2): 124–30.
26 Piscitelli P, Barba M, Crespi M, Di Maio M, Santoriello A, D’Aiuto M, et al.; Human Health Foundation Study Group, in memory of Prof. Giovan Giacomo Giordano. The burden of breast cancer in Italy: mastectomies and quadrantectomies performed between 2001 and 2008 based on nationwide hospital discharge records. J Exp Clin Cancer Res. 2012 Nov; 31(1): 96.
27 Huff L, Bogdan G, Burke K, Hayes E, Perry W, Graham L, et al. Using hospital discharge data for disease surveillance. Public Health Rep. 1996 Jan-Feb; 111(1): 78–81.
28 Schneider N, Dreier M, Amelung VE, Buser K. Hospital stay frequency and duration of patients with advanced cancer diseases - differences between the most frequent tumour diagnoses: a secondary data analysis. Eur J Cancer Care (Engl). 2007 Mar; 16(2): 172–7.
29 Bredenberg PA, Lagoe RJ. Mastectomies for malignancy: a DRG-based hospital utilization analysis. J Surg Oncol. 1987 May; 35(1): 19–23.
30 Pollock AM, Vickers N. Deprivation and emergency admissions for cancers of colorectum, lung, and breast in south east England: ecological study. BMJ. 1998 Jul; 317(7153): 245–52.
31 Scheller-Kreinsen D, Quentin W, Geissler A, Busse R; EuroDRG Group. Breast cancer surgery and diagnosis-related groups (DRGs): patient classification and hospital reimbursement in 11 European countries. Breast. 2013 Oct; 22(5): 723–32.
32 Instituto Nacional de Estatística. População residente (n.o) por local de residência, sexo e grupo etário, anual. 2019 (cited 2019 Apr 17). Available from: https://www.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_indicadores&i ndOcorrCod=0004163&xlang=pt&contexto=bd&selTab=tab2. [ Links ]
33 Sondik EJ. Breast cancer trends. Incidence, mortality, and survival. Cancer. 1994 Aug; 74(3 Suppl): 995–9.
34 Cancer Research UK. Breast cancer incidence (invasive) statistics. 2020 (cited 2017 Jul 4). Available from: http://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/breast-cancer/incidence-invasive. [ Links ]
35 Keegan TH, Chang ET, John EM, Horn-Ross PL, Wrensch MR, Glaser SL, et al. Recent changes in breast cancer incidence and risk factor prevalence in San Francisco Bay area and California women: 1988 to 2004. Breast Cancer Res. 2007; 9(5):R62. [ Links ]
36 André MR, Amaral S, Mayer A, Miranda A, Ror Sul WG; ROR SUL Working Group. Breast cancer patients survival and associated factors: reported outcomes from the Southern Cancer Registry in Portugal. Acta Med Port. 2014 May-Jun; 27(3): 325–30.
37 Levi F, Te VC, Maspoli M, Randimbison L, Bulliard JL, La Vecchia C. Trends in breast cancer incidence among women under the age of forty. Br J Cancer. 2007 Oct; 97(7): 1013–4.
38 Anders CK, Johnson R, Litton J, Phillips M, Bleyer A. Breast cancer before age 40 years. Semin Oncol. 2009 Jun; 36(3): 237–49.
39 Botha JL, Bray F, Sankila R, Parkin DM. Breast cancer incidence and mortality trends in 16 European countries. Eur J Cancer. 2003 Aug; 39(12): 1718–29.
40 Colonna M, Delafosse P, Uhry Z, Poncet F, Arveux P, Molinie F, et al.; FRANCIM Network. Is breast cancer incidence increasing among young women? An analysis of the trend in France for the period 1983-2002. Breast. 2008 Jun; 17(3): 289–92.
41 Merlo DF, Ceppi M, Filiberti R, Bocchini V, Znaor A, Gamulin M, et al.; AIRTUM WG. Breast cancer incidence trends in European women aged 20-39 years at diagnosis. Breast Cancer Res Treat. 2012 Jul; 134(1): 363–70.
42 Barchielli A, Paci E. Trends in breast cancer mortality, incidence, and survival, and mammographic screening in Tuscany, Italy. Cancer Causes Control. 2001 Apr; 12(3): 249–55.
43 Leclère B, Molinié F, Trétarre B, Stracci F, Daubisse-Marliac L, Colonna M; GRELL Working Group. Trends in incidence of breast cancer among women under 40 in seven European countries: a GRELL cooperative study. Cancer Epidemiol. 2013 Oct; 37(5): 544–9.
44 Dijkstra L, Poelman H. Regional working paper 2014: a harmonised definition of cities and rural areas: the new degree of urbanisation (WP01/2014) (Internet)Brussels: European Commission; 2014., Available from http://ec.europa.eu/regional_policy/sources/docgener/work/2014_01_new_urban.pdf
45 Ellis L, Woods LM, Estève J, Eloranta S, Coleman MP, Rachet B. Cancer incidence, survival and mortality: explaining the concepts. Int J Cancer. 2014 Oct; 135(8): 1774–82.
46 Eurostat. In-patient average length of stay (days) by NUTS 2 regions, females. 2018 (cited 2019 Apr 10). Available from: http://appsso.eurostat.ec.europa.eu/nui/show.dodataset=hlth_co_inpstf&lang=en. [ Links ]
47 Eurostat. Hospital discharges by diagnosis, in-patients, per 100,000 inhabitants. 2019 [cited 2019 Aug 7). Available from: http://appsso.eurostat.ec.europa.eu/nui/show.do?dataset=hlth_co_disch2&lang=en. [ Links ]
48 Gomes I, Miranda A, Nunes C. Spatiotemporal analysis of breast cancer incidence: a study in Southern Portugal between 2005 and 2012. Anticancer Res. 2018 Mar; 38(3): 1797–805.
49 Allemani C, Weir HK, Carreira H, Harewood R, Spika D, Wang XS, et al. Global surveillance of cancer survival 1995–2009: analysis of individual data for 25,676,887 patients from 279 population-based registries in 67 countries (CONCORD-2). Lancet. 2015; 385(9972): 977–1010.
50 Allemani C, Matsuda T, Di Carlo V, Harewood R, Matz M, Nikšic M, et al.; CONCORD Working Group. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet. 2018 Mar; 391(10125): 1023–75.
Acknowledgment
We thank the ACSS for kindly providing the data for this study.
Statement of Ethics
This is not required as the database used was anonymized prior to data collection.
Conflict of Interest Statement
The authors have no conflict of interests to declare.
Funding Sources
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sector.
Author Contributions
All of the authors contributed to the study conception and design.Material preparation, data collection, and analysis were performed by Inês Afonso Gomes and Bruno Moita. The first draft of this paper was written by Inês Afonso Gomes, and all authors commented on previous versions of this paper. All of the authors read and approved the final version of this work.

