











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkThe overstretched intensive care unit (ICU) capacity during the 2019 coronavirus disease (COVID-19) pandemic generated a debate about age being an important criterion for triaging patients with COVID-19 for ICU admission [1,2].
In Portugal, as of April 30, 2020, there have been 24,987 cases of severe acute respiratory syndrome coronavirus 2 (SARS-CoV2) infection (6,136 [24.5%] patients aged ≥70 years) and 1,007 individuals have died from COVID-19 (878 [87.2%] patients aged ≥70 years) [3,4].
This was a multicenter retrospective cohort using data retrieved from the ICU databases. For comparisons between variables, we used χ2or Fisher exact tests (SPSS V20; IBM Corp., North Castle, NY, USA).
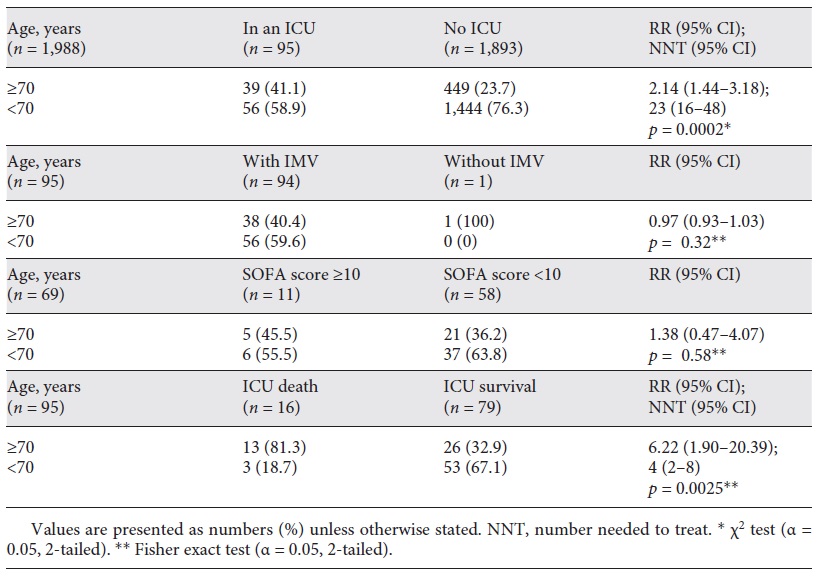
As of April 30, in 6 hospitals in Lisbon (catchment area of 1.2 million people), 95 (4.8% of a total of 1,988 cases) patients with COVID-19 pneumonia (nasal/pharynx swab or respiratory secretions with positive SARS-CoV2 by real-time polymerase chain reaction) were admitted to the ICU, with 39 (41.1%) patients aged ≥70 years. Overall, 94 (98.9%) patients required invasive mechanical ventilation (IMV). Among those aged ≥70 years, 38 (97.4%) patients required IMV and only 1 (2.6%) patient was managed solely with a high-flow nasal cannula. Overall, the mean (±SD) sequential organ failure assessment (SOFA) score on ICU admission was 7 (±3), and 16 (16.8%) patients did not survive the ICU stay.
Four ICU (70.5% of the 95 patients included) were using the Clinical Frailty Scale to help triage patients with COVID-19 for ICU admission, with those having >6 points being generally declined for ICU care [5]. In 5 (12.8%) patients aged ≥70 years, do-not-resuscitate decisions were established during the ICU stay.
In this cohort, patients aged ≥70 years were twice more likely to be admitted to the ICU than others (Table 1; RR = 2.14; 95% CI 1.44-3.18). Moreover, patients aged ≥70 years had access to IMV (RR = 0.97; 95% CI 0.93-1.03) and mean SOFA scores similar to those of others (8 vs. 7; RR = 1.38; 95% CI 0.47-4.07). However, patients aged ≥70 years were 6 times more likely to die in the ICU than others (RR = 6.22; 95% CI 1.90-20.39). Alternatively, of every 4 patients aged ≥70 years admitted to the ICU, 1 derived a survival benefit from ICU care (number needed to treat: 4; 95% CI 2-8).
Our findings suggest that chronological age was not a limitative criterion for ICU admission in patients with COVID-19. More likely, clinicians pondered factors such as the number and severity of comorbidities, the presence and severity of frailty, and the number and severity of acute organ dysfunctions [5].
The following limitations warrant consideration. First, the COVID-19 incidence decreased a few weeks following the lockdown imposed by the Portuguese government on March 18 (from a peak of 1,516 cases on April 10 to 368 cases on April 30) [3]. Second, the peak ICU bed occupancy rate occurred on April 6 (60.1% of the total national capacity) [4]. Finally, data on comorbidities and patients declined for ICU admission were not captured and thus we could not weigh for those potential confounders.
In conclusion, access to ICU care for elderly patients with COVID-19 may be preserved during the pandemic, especially if there is no strained ICU capacity. While patients aged ≥70 years may incur in a higher mortality, those selected by ICU clinicians may benefit from ICU care.

