











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
About 50 million people worldwide lived with dementia in 2018, with a new case being diagnosed every 3 seconds. Projections estimate that in 2030 that number will have increased to 82 million people, reaching 152 million people in 2050 [1]. In Portugal, it is estimated that 182,000 people live with dementia [2], with about 19.9 cases per 1,000 inhabitants, being the country with the fourth highest number of cases in the world [3]. In advanced stages, people with dementia (PwD) may experience feeding difficulties, usually manifested by oropharyngeal dysphagia, refusal to eat, and aversive behaviors, among others [4, 5].
The Edinburgh Feeding Evaluation in Dementia Scale (EdFED) [6] is a widely validated scale that measures feeding difficulties in PwD based on their eating behaviors [7-11]. The EdFED can detect feeding difficulties even in people with severe cognitive impairment, when the usual instruments are less effective in detecting functional decline [12]. It is a 10-item questionnaire, easy and quick to apply, which assesses and monitors changes in PwD eating behavior. The first two items refer to the need for assistance during meals. Items 3 and 4 are indicators of the person’s difficulty in feeding herself/himself. Items 5-10 describe feeding behaviors, ranging from refusing food to keeping the mouth open while eating [10]. Each item is scored according to the frequency of its occurrence during the meal: 0 if the behavior never happens, 1 if it happens sometimes, and 2 if it happens often. The final score ranges from 0 to 20. A higher score indicates higher impairment [12].
Studies of psychometric properties showed that the EdFED has a high internal consistency (Cronbach’s α = 0.87), validity of construct, as well as inter- and intrarater reliability (r = 59, p = 0.013 and r = 0.95, p < 0.000, respectively) [13].
The instrument has the same precision when measuring behaviors through direct observation or the caregiver’s report [12]. It is recommended by the European Society for Clinical Nutrition and Metabolism to identify eating problems and behavioral symptoms in PwD [14] and is also considered by the Hartford Institute of Geriatric Nursing, New York University as the best tool to assess feeding difficulties in older PwD [15]. Currently, there are validated versions for traditional and simplified Chinese [7, 8], Spanish [9], French [10], and Italian [11]. However, there is no European Portuguese version of the EdFED.
The main objective of this study was to translate and adapt the EdFED into the Portuguese language. Second, the study aimed to evaluate its psychometric properties (internal consistency and interobserver reliability) in a sample of Portuguese institutionalized PwD. Finally, a brief characterization of the feeding difficulties presented by the studied sample was carried out.
Subjects and Methods
Design and Participants
An observational, transversal, exploratory-descriptive study was conducted with a convenience sample of institutionalized PwD between July and December 2019. First, the EdFED was translated, culturally adapted, and linguistically validated. Then, a study of its psychometric properties was developed, namely internal consistency and interobserver reliability. Participants were selected from nursing homes in the central region of Portugal. The inclusion criteria were (1) ≥65 years old, (2) diagnosis of dementia recorded in the clinical file, (3) institutionalization for at least 2 months, (4) feeding difficulty requiring supervision and/or direct help during meals identified and reported by the nursing home director and/or nurses in charge, and (5) presence of a legal proxy to sign the consent form. Those who fed independently as well as those who were fed exclusively by nasogastric tube or gastrostomy were excluded.
Translation and Adaptation Procedures
Permission for the development of the European Portuguese version of the EdFED was obtain from its author, Dr. Roger Watson. The linguistic validation process followed the principles of good practice for translation and cultural adaptation proposed by the International Society for Pharmacoeconomics and Outcomes Research [16]. First, a translation into the Portuguese language was done by the first author of this study, who has good skills of the English language and professional knowledge in health, aging, dementia, and feeding. Then, a reconciliation was made by the co-authors of this study. After review, adaptation of the initial translation, and discussion for consensus, the first version of the EdFED-PT was obtained. A retroversion into English was performed by a faculty professor whose mother language is English but who has advanced knowledge of European Portuguese. For harmonization, all translators compared versions, with item-by-item analysis, resulting in version 2 of the EdFED-PT. In the cognitive debriefing stage, whose main objective was to check the understandability, interpretation, and cultural relevance of the translation [16], an expert panel with health professionals and/or faculty teachers/researchers was formed to analyze the translation of the EdFED. The group analyzed each item in order to verify their understanding and meaning, thus reducing the ambiguity of understanding. With the conclusion of this analysis, version 3 of the EdFED-PT was created. Finally, an orthographic revision of version 3 was done by a Portuguese language teacher for possible corrections, giving rise to the final version of the EdFED-PT.
For the cognitive debriefing, eight health professionals and/or faculty teachers/researchers were invited in a nonprobabilistic convenience sample. The choice was made due to the knowledge on the subject of the study, academic degree, and experience in the referred area and respective target population. Regarding profession, the sample consisted of one social worker, one nurse, three gerontologists, one psychologist, and two speech therapists.
Each expert was instructed to assess the degree of agreement between the original version and the translation synthesis, observing the aspects of semantic, idiomatic, and experiential or cultural equivalence, and had to indicate the degree of agreement between the original version and the synthesis of the translation of each item of the EdFED on a scale from 1 to 4, which corresponds to 1 = disagree, 2 = slightly agree, 3 = agree, and 4 = totally agree. When grades 1 or 2 were marked, experts were asked to justify their choice and to write down observations and suggestions in a specific field. An agreement of 80% was stipulated to determine consensus among the experts, and the items with lower agreement were re-evaluated in a second round, considering the information of what was not consensual in the group’s opinion, and they were able to maintain or modify their opinion.
For the analysis of content validity, the criteria proposed by Polit and Beck [17] were followed, through the content validity index (CVI), which measures the degree of satisfaction of the panel of experts when evaluating an instrument, and it is calculated by adding the items measured as 3 or 4 to be divided by the total number of responses. The probability of change and modified κ was also calculated, which is a consensus index of the agreement between the evaluators that complements the CVI, removing the random chance agreement [18].
Assessment of the Psychometric Properties of the EdFED-PT
This phase of the study was performed in six nursing homes in central Portugal and consisted of the application of the EdFED-PT. The behavior of 51 PwD was observed during lunch. The meals of 40 participants (mean age 85.77 ± 7.15 years, 87.5% female) were observed simultaneously by the main researcher and a psychologist with academic formation in gerontology and geriatrics and well-versed in the use of the instrument, in order to analyze the interobserver reliability.
Statistical Analysis
For sample characterization, descriptive statistics were used through the calculation of absolute frequencies and measures of central tendency and dispersion (mean and standard deviation). Internal consistency was assessed by Cronbach’s α, and it is considered very good at >0.9, good at 0.8-0.9, reasonable at 0.7-0.8, weak at 0.6-0.7, and inadmissible at <0.6 [19]. The interobserver reliability assessment was carried out by Cohen’s κ, whose values vary between 0 and 1, and although there is some variation in the interpretation of its values, the proposal by Landis and Koch [20] is one of the best-accepted: <0 = poor, 0.00-0.20 = weak, 0.21-0.40 = considerable, 0.41-0.60 = moderate, 0.61-0.80 = substantial, and 0.81-1.00 = almost perfect. The percentage of agreement between the observers was also calculated.
In inferential statistics, for the study of the relationship between sociodemographic variables and the total EdFED score, nonparametric tests were chosen: Mann-Whitney U test for comparison of two independent categories and Spearman’s coefficient to verify the degree of relationship between two variables. Inferential results <0.05 were considered significant. Analysis of the results was performed with the support of the SPSS statistics software (IBM Corp., Armonk, NY, USA) version 25.
Results
Content Validity
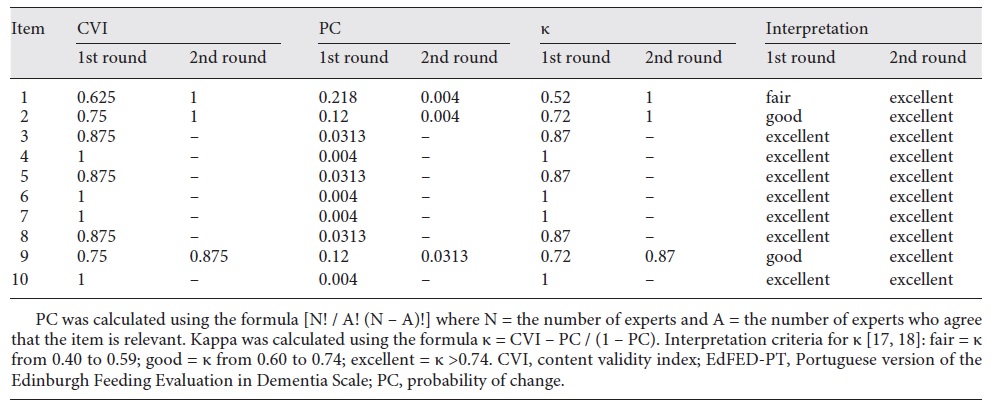
At the end of the first evaluation round, three items from the EdFED-PT had a CVI <0.8. After the second round, two items had a CVI of 1 and the other had a CVI of 0.875. The mean value of the CVI at the end of the evaluations was 0.950. The probability of change values varied between 0.004 and 0.0313. The modified κ varied between 0.52 and 1, with a mean κ value of 0.94, being considered excellent (Table 1). After the two rounds no expert suggested any changes in the translations that pointed to the need of cultural adaptations.
Participants
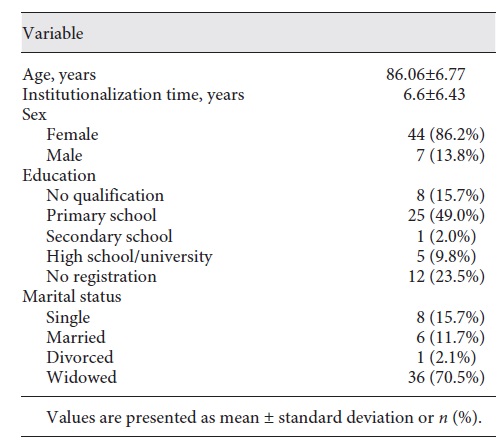
A total of 51 institutionalized PwD participated in this study. The mean age was 86.06 ± 6.77 years and the majority were women (n = 44, 86.2%). Most participants were widowed (n = 36, 70.5%) and had a low academic qualification (Table 2).
Internal Consistency
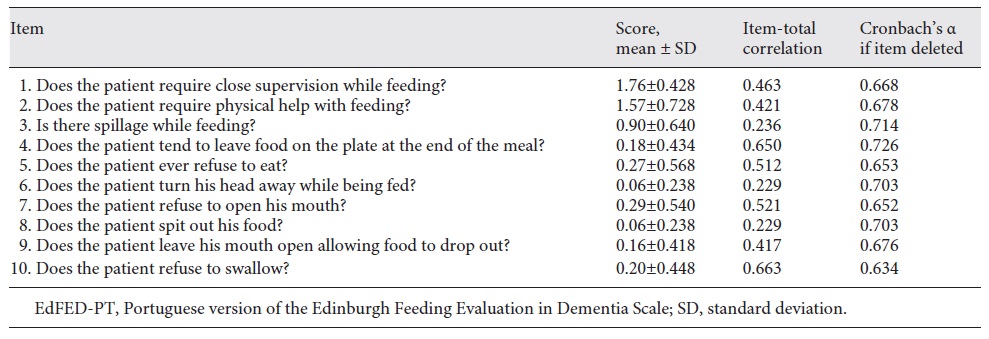
To verify the internal consistency of the EdFED-PT, Cronbach’s α was calculated, obtaining a total score of 0.705. Items 6 and 8 show the lowest item-total correlation scores (0.229) and item 10 the highest one (0.663) (Table 3).
Interobserver Reliability
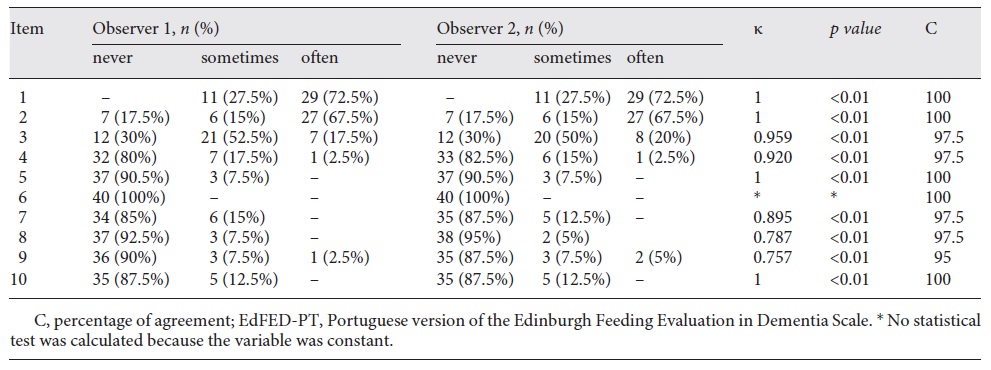
For the study of EdFED-PT interobserver reliability, a sample of 40 PwD was considered. The value of the total Cohen’s κ obtained was 0.882 and the percentage of agreement between the observers was 98.5% (Table 4).
Study of Feeding Difficulties
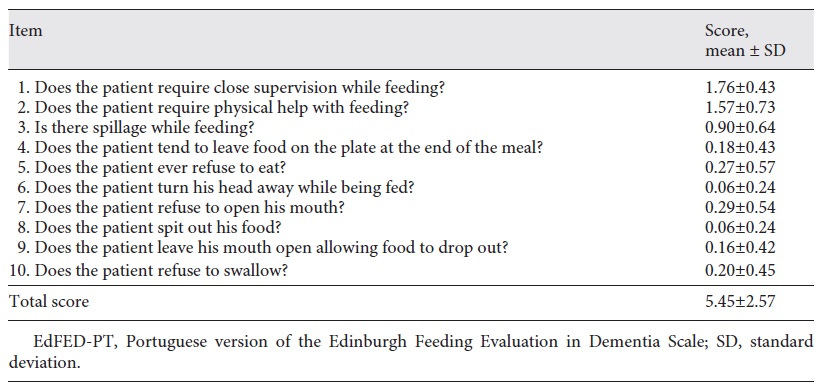
The mean total score among the 51 participants was 5.45 ± 2.57 (Table 5). The items with the highest score were item 1 (1.76 ± 0.43) and item 2 (1.57 ± 0.73). These items showed the need for assistance during meals and averaged 1.66 ± 0.58. Items 3 and 4, indicators of the person’s difficulty in eating alone, averaged 0.54 ± 0.53. Items 5-10, which describe the behaviors that reflect signs of functional or cognitive decline, had an average value of 0.17 ± 0.41.
There were no statistically significant correlations or differences between the final EdFED-PT score and PwD age (rs = -0.01, p = 0.946), sex (U = 109.5, p = 0.219), or institutionalization time (rs = 0.221, p = 0.119).
Discussion and Conclusion
This study aimed to contribute to the adaptation of the EdFED to the Portuguese population. It was intended to analyze its internal consistency and interobserver reliability, in addition to characterizing the feeding difficulties of institutionalized PwD, including an analysis of the relationship between the participants’ sociodemographic variables and the results of the EdFED.
From the cultural and linguistic translation and validation phase, the appropriate version for the Portuguese population emerged, with a CVI of 0.950. This value is in accordance with that recommended in the literature, which suggests values >0.8 when the panel of experts is composed of more than six subjects [17, 21], and that in checking the validity of new instruments the values recommended by Polit and Beck [17] must be >0.900. Although other EdFED translation and adaptation studies used retroversion processes followed by expert evaluation, only the Chinese versions evaluated the content validity by calculating the CVI, obtaining values of 0.969 for traditional Chinese (Taiwan) and 1.0 for simplified Chinese (Mainland China) [7, 8].
Content validity refers to the degree to which each item is relevant and representative of a construct with a specific objective of evaluation and is fundamental in the process of developing or adapting evaluation instruments [22-25]. The CVI measures the proportion of experts who are in agreement on the items of the instrument, and when its value is ≥0.800 in all items evaluated, the validation process is concluded [26].
During the cultural adaptation of the instrument, the evaluation by the panel of experts was a crucial point to guarantee the robustness of the process. Attention should be paid to the number and qualification of the experts, and some authors recommend 5-10 experts [21] and others suggest a minimum of 6 up to 20 experts [22].
According to the instrument’s characteristics and theme, the academic graduation, qualification, and availability of the participants must be considered, who must have clinical and/or research experience in the theme, and when dealing with a process of cultural adaptation, formation of a multidisciplinary commission is suggested [26]. The group of eight experts formed for this study had professionals with a high academic level (all PhD) in different areas, from social sciences to health sciences, with experience in the field of aging and/or dementia, and contributed to obtaining a global, judicious, and credible assessment. The group’s specialization and multidisciplinarity were essential for the rigor in the validation process, since dementia requires varied and specific knowledge. Specifically, the presence of nurses, speech therapists, and gerontologists were an asset, given that these professionals deal directly with the issues of aging and also with feeding.
After the EdFED’s external evaluation, with content evaluation using an expert panel, internal evaluation was performed through the study of its psychometric properties. These are parameters that indicate the quality and scientific value of the results obtained after the application of an evaluation instrument [27]. Due to the importance of the assessment instrument for both research and clinical practice, studying its qualities is essential to ensure that the researchers and/or professionals will have consistent tools at their disposal [27].
The EdFED-PT showed reasonable internal consistency (Cronbach’s α = 0.705) according to the criteria of Pestana and Gageiro [19]. Exclusion of any of the 10 items would not increase the α value. Other authors established different values for the classification of Cronbach’s α, such as DeVellis [28], who considers an α value between 0.70 and 0.80 to be respectable. In exploratory studies, the α value may decrease to 0.60 [29], provided that the results obtained are interpreted with caution [30].
The internal consistency defined by calculating Cronbach’s α was evaluated in studies of the original, Spanish, and Chinese versions. Therefore, despite having a lower value than those found in the original version (α = 0.870) [31], the Spanish version (α = 0.880) [9], the simplified Chinese version (α = 0.910) [7], and the traditional Chinese version (α = 0.900) [8], it is possible to consider that the EdFED-PT has satisfactory internal consistency. However, in these studies the sample size was >100 PwD, twice the sample in this study (51 participants). It is standardized to have at least 10 participants per item of the instrument. In this study, for each item five participants were obtained, with a minimum recommended value [29]. Additionally, according to Conroy [32], samples >30 can already reliably measure an α value. Future studies should increase the sample size to measure the values of internal consistency and allow a more accurate comparison with the other validation studies.
Regarding the study of the EdFED-PT’s interobserver reliability, the results were quite satisfactory. There was almost perfect agreement between the observers [20]: Cohen’s κ = 0.882 and 98.5% agreement. In the EdFED’s previous translation studies, interobserver reliability was analyzed in the English, Spanish, and simplified Chinese versions, which obtained good results. However, the methodology was different from the one chosen for the present study. Pearson’s correlation was used in the English [33] and simplified Chinese [7] versions, obtaining r = 0.59 (p = 0.013) and r = 0.81 (p < 0.0001), respectively. In the Spanish version [9] the authors evaluated interobserver reliability by calculating the intraclass correlation coefficient between observations made by nurses and professional caregivers (0.94, p < 0.0001), nurses and family caregivers (0.81, p < 0.0001), and between professional caregivers and family caregivers (0.78, p < 0.0001). Although it was stipulated by a different method, this study demonstrated that the EdFED-PT also has satisfactory interobserver reliability.
The methodology used in each EdFED translation and validation study was different, as was the sample of each one. Samples of PwD ranged from 26 in the Canadian study [10] to 262 in the Spanish translation [9]. The mean age of the PwD in the present study was 86.06 ± 6.77 years, slightly higher than the average age of previous studies (80.82 ± 10.02 years). The probability of increasing the severity of dementia as well as the need for institutionalization and mortality vary according to age and dementia stage [34]; therefore, within about 5 years, which was the difference in the mean of age between studies, the trajectory of dementia can cause differences in symptoms with advancing age. A predominance of the female sex occurred in this and other validation studies [7-11], being slightly higher in the current research: 86.2 vs. 76.5% of women. Two-thirds of clinically diagnosed dementia cases are in women [35]. This is justified by the fact that women have greater longevity and are thus more susceptible to developing the condition.
In addition to the exploratory study of the EdFED-PT’s psychometric properties, this study was valued with the application of the instrument to a group of institutionalized PwD in order to characterize their feeding difficulties.
Participants had an average EdFED-PT score of 5.45. The items with the highest score were item 1 (1.76) and item 2 (1.57), indicating that the sample has a great need for assistance at the time of the meal. There were some behaviors indicative of functional and cognitive decline, with refusal to eat and to open the mouth being the ones that occurred most frequently. The fact that the observation occurred in just one meal limits the result of the assessment to the behavior of the PwD at that time. Participants who performed well at the time of observation could be on a “good” day, when the PwD was to have more difficulty with meals. The opposite situation can also occur, when a person who usually eats with great difficulty performed well at the time of observation. An evaluator who had more knowledge of both the instrument and the person to be observed could increase the likelihood of a more reliable assessment.
Sociodemographic variables (age, sex, and length of institutionalization) were not significantly associated with feeding difficulties of older PwD in this study. A probable explanation for these results may be due to the possibility of having in the sample people with different stages of dementia, since dementia itself implies a trajectory with some unpredictability. A better characterization of the type and degree of dementia in future studies could point to some relationship between the stage of dementia and the result obtained at EdFED.
The main limitation of this study focuses on the fact that the sample was small, which compromises the generalization of the results to the Portuguese institutionalized population with dementia. Although the institutions that participated in this study had an occupancy rate of 100%, a limitation in the selection of participants was underrecording of the diagnosis of dementia in the clinical process. This factor contributed to reducing the number of participants, as this was one of the main inclusion criteria. Another limitation was the absence of more data regarding the type and degree of dementia recorded in the clinical process of the participants. The history of the disease was, in most cases, not very detailed. In future studies, it is suggested that the application of assessment instruments better characterize the participants’ cognitive and functional status.
Furthermore, validation analyses (e.g., construct validity) were not possible due to the small sample size. The adapted Portuguese version of the EdFED and its reliability analysis were a first step to providing a tool that allows assessing the feeding difficulties experienced by PwD and provides early-action solutions other than standard practice in this situation. Nevertheless, a confirmatory factor analysis of this version is needed, and further studies should test the replicability of the three-factor model, qualities, and proportions of the original EdFED.
Another limitation was the use of data analysis methodology different from that used in the translation and validation of the EdFED into other languages, thus making it difficult to compare the results.
Future studies could correlate the final score with a nutritional assessment scale to explore if, or how, the feeding difficulties presented are related to nutritional status and caloric intake. Studies evaluating other psychometric properties, such as intraobserver reliability, would also increase the knowledge about EdFED-PT psychometric properties.
Conclusion
The main objective of this study was to contribute to translation and adaptation of the EdFED to the Portuguese population, in addition to studying some of its psychometric properties and analyzing the relationship between sociodemographic variables and the results of the scale. By strictly following the content validation procedure and conducting an exploratory study of psychometric properties, the main results suggest that the EdFED-PT allows to recognize feeding difficulties in institutionalized older PwD.
The EdFED-PT is considered a reliable instrument, and in addition to its assistance to determine the level of impairment as well as to evaluate the need of multidimensional intervention in feeding of older adults with dementia, it also allows comparison with international studies that use the EdFED as an evaluation tool.

