











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
The COVID-19 global pandemic caused by the virus SARS-CoV-2 has been ravaging the world since it was first identified in Hubei, China, in December 2019 1. Since then, it has, at the time of writing (December 2021), infected over 265 million people and caused more than 5.2 million deaths worldwide 2.
The virus can be transmitted directly in a person-to-person fashion through droplets or aerosols expelled by the infected person or indirectly through the contact of susceptible individuals with objects that have been contaminated by those particles 3. Thus, the context in which the contact occurs ends up being pivotal for the spreading capacity of the virus. Physical proximity, especially when under 1.5-2 m, is a preponderant factor for the transmission, as well as when it occurs in small, closed, and poorly ventilated spaces. The duration of the contact is another important factor. The longer the contact lasts, the higher the risk of transmission. Conversely, restricting the duration of contact between individuals, their occurrence in large, well-ventilated spaces, the maintenance of distances greater than 2 m, the promotion of mask usage, and frequent hand washing are associated with a mitigated spreading of the virus 4,5.
From a public health perspective, interventions need to be focused on reducing factors known to be associated with higher virus transmission and promoting those that restrain it. Thus, it is of pivotal importance to have an epidemiological surveillance system in place, to perform epidemiological inquiries into all positive cases, isolate them, as well as identify and isolate their high-risk contacts 4. Measures taken at the international and national levels, like travel restrictions and general lockdowns, also help curb virus spread. Furthermore, it has been shown that, as far as the impact of the pandemic on economies goes, countries with higher yearly investments in healthcare, of about 7.6% of GDP or about USD 2,300 per capita, have lower average COVID-19 fatality rates, allowing for a shorter duration of lockdowns, and consequently less GDP shrinkage 6,7. The countries that have had better performances in dealing with the pandemic as measured by indexes of resilience, preparedness, and prevention were also those with higher levels of health expenditures, averaging 8.6% of GDP, and higher indexes of public governance 8. Alternatively, certain environmental factors, along with suboptimal investments in healthcare, have shown to be important contributing factors to COVID-19 morbidity and mortality. Cities with more than 100 days exceeding the limits set for PM10 or ozone, little wind, and lower average temperatures have seen a greater number of infected individuals and a higher death toll 9. On the other hand, cities with lower exposure of the population to days exceeding safe levels of PM2.5 have shown a lower average fatality rate 7.
The pandemic has exerted tremendous pressure on most countries’ national health systems, and Portugal was no exception. With more than 1 million confirmed cases and over 18,000 reported deaths since the beginning of the pandemic 10, Portuguese healthcare professionals found themselves in a situation where they had to work extended shifts, with no weekend breaks or days off for weeks on end, so the high demand of health services caused by the COVID-19 crisis could be met. This was also the case with Public Health Medical Residents (PHMR). According to the World Health Organization, burnout is a syndrome resulting from prolonged exposure to work-related stress and is mainly characterized by feelings of depletion or exhaustion, increased mental and emotional distance from one’s job, feelings of negativism or cynicism related to one’s job, and reduced professional efficacy. It refers specifically to phenomena in the occupational context 11. A 2019 meta-analysis by Koutsimani et al. 12 states that, although burnout and depression are different constructs, they correlate by 0.75. Despite not being a recognized mental illness in the 5th edition of the Diagnostic Statistical Manual of Mental Disorders 13, burnout can affect the global health of the individual and be responsible for an increased demand for health services 11.
Burnout is a concept firstly described in 1974 by Freudenberger 14 as comprising a series of unspecified physical and psychological symptoms, produced by an excessive energy requirement at work, and usually occurring among professions involving a helping relationship. Burned-out individuals were described as beset by physical symptoms such as headache and daytime sleepiness, and as demonstrating irritability and a rigid thought pattern. Burned-out workers looked and acted as if they were depressed 14. Maslach and Leiter 15 expanded the concept of burnout and redefined it as a crisis in relationships with work and not necessarily a crisis with work people. According to these authors, burnout is defined as a syndrome with three dimensions: emotional exhaustion (EE), depersonalization (DP), and a lack of personal accomplishment (PA) at the workplace, which arise when functional coping strategies fail 16.
According to Maslach et al. 17, the risk factors for burnout can be divided into 7 categories: workload, control, reward, community, fairness, values, and job-person incongruity 18,19. Workload pertains to the overload felt by professionals when job demands exceed human limits. This risk factor is more closely related to the exhaustion dimension 20,21 that mediates the relationship between workload with DP and lack of PA 22,23. Overload contributes to exhaustion by depleting the capacity of people to meet the demands of the job and gets to a critical point when there is no opportunity to recover during restful periods at either work or home 24. Conversely, a sustainable workload allows for the effective use and improvement of existing skills, and for the worker to become proficient in new areas of activity 25.
Lack of control in the work setting has also been linked to the development of burnout. Patient noncompliance, inability to manage scheduled work hours, and not being allowed to participate in organizational decisions are examples of lack of control in healthcare 26. Another important factor in this realm is the lack of job resources, which has been found to contribute to workers’ disengagement 22. Role ambiguity and role conflicts are also associated with greater burnout, as well as the absence of direction in the workplace 17,20. Conversely, active participation in organizational decision-making, and clearly defined roles and expectations from organizational leadership are associated with better levels of efficacy and lower levels of exhaustion and burnout 27,28.
Insufficient reward, be it financial, institutional, or social, when compared to expectations has been shown to increase people’s vulnerability to burnout 29,30. Lack of recognition from service recipients, colleagues, managers, and external stakeholders undermines both the work and the workers, and is associated with feelings of inefficacy 17,20. On the other hand, when consistency between the person and the job in the reward dimension is present, the likelihood of there being intrinsic satisfaction is higher 31.
Community refers to the overall quality of social interactions at work, and this includes themes such as conflict, mutual support, closeness, and the ability to work as a team. Burnout is less likely to occur within a positive and supportive work environment 32.
Fairness is the extent to which decisions at work are regarded as being fair and equitable 18. Employees who perceive their supervisors as being both fair and supportive are less susceptible to burnout and are more accepting of major organizational change 33.
Values refer to the emotional and cognitive power of job goals and expectations. They are the ideals and motivations that attracted people to their jobs and are the motivating connection between the worker and the workplace, going beyond the mere exchange of time for money 18. Conflict in values is related to all three dimensions of burnout 34.
Lastly, job-person incongruity refers to the problematic relationship between the person and the environment, which is frequently referred to as imbalance, misalignment, or misfit. This incongruity can be observed when the demands of the job exceed the capacity of the individual to cope effectively, or the person’s efforts are not reciprocated with equitable rewards 18. According to Maslach and Leiter’s 15 burnout model, the greater the perceived incongruity, or mismatch, between the person and the job, the greater the likelihood of burnout.Conversely, the greater this congruity is, the greater the likelihood of engagement with work.
Burnout has been linked to a variety of consequences, either physical, psychological, or occupational. A 2017 meta-analysis of 36 articles by Salvagioni et al. 35 found that the burnout syndrome is associated with coronary heart disease 36 and hospitalization for cardiovascular diseases 37, and their risk factors such as obesity, hyperlipidemia, type 2 diabetes, large waist circumference, high body mass index, metabolic syndrome, hypertension, high triglycerides, low HDL cholesterol, high LDL cholesterol 38, and fasting hyperglycemia 39. In terms of physical symptoms, it has also been associated with musculoskeletal pain 40, changes in pain experience 41, prolonged fatigue 42, gastrointestinal issues, respiratory problems 43, severe injuries 44, and increased mortality below 45 years of age 45.
Regarding psychological issues, burnout is associated with increased insomnia 46 and sleep disturbances 43 and is a predictor of depressive symptoms 47, higher risk of initiating antidepressant treatment among men 48, and hospital admissions due to mental disorders 37. Burnout also affects the quality of work. EE and DP are predictors of job dissatisfaction 49, and burnout is associated with increased sickness absence days (21%) and sickness absence spells (9%) 50. Burnout is also a risk factor for leaves due to musculoskeletal disorders, and disorders of the circulatory and respiratory systems 51. It has been found to predict new disability pensions during a 4-year follow-up in a Finnish study 44.
During the pandemic, PHMR’s main functions were, among other things, interviewing confirmed cases and collecting information on the clinical history and possible contacts, performing contact tracing, and classifying them as high-risk exposure (close) contacts or low-risk exposure contacts. This was made to test and quarantine those contacts at high risk of having contracted the virus and, hopefully, break the transmission chain of infection 52. PHMR also had to manage outbreaks at institutions such as schools and long-term care facilities. The high demand for health services during the pandemic has increased the workload placed upon these professionals. Some of them had to work 12-16 h every day for several months, with virtually no time left for themselves or their families. The increasing wave of new COVID notifications might have left some of them with an acute sense of lack of control regarding the amount of work that would be expected of them on any given day, as well as the fact that their interventions seemed to have little or no impact on the incidence of the disease - due to a lack of human resources, during high incidence periods most new cases and their contacts were isolated only several days after the onset of symptoms or diagnosis. This fact may also have led to an internal conflict of values, leading some of them to believe that part of that hard work was futile and to wonder whether, instead of merely acting by protocol, their time should be allocated to other tasks for better effectivity in dealing with the pandemic.
All these factors could have contributed to the emergence of burnout among PHMR, and, if that is the case, measures such as hiring more medical personnel or optimizing the process of epidemiological surveillance must be taken. These actions should mitigate the effects of burnout on these professionals and protect their mental health, as well as better prepare public health services to better deal with future pandemics. One must first assess, however, the levels of burnout in this population. With this study, thus, we aimed to evaluate the prevalence of burnout among PHMR.
Materials and Methods
Sample and Data
Public health doctors’ interventions are usually of a populational scope, unlike other medical specialities, whose focus is the individual patient. These include population health status assessment, health planning and management for health promotion, protection, and disease prevention, health authority functions, and surveillance and monitoring of transmittable and nontransmittable diseases. During the pandemic, their main functions were team management, data collecting and processing, epidemiological surveillance, and isolation of COVID-19-positive cases and their contacts. Due to understaffing problems among Public Health Units, PHMRs have to take on most of these activities, with very little support from their superiors, who were also overwhelmed. All the Portuguese PHMRs (out of around 200) were invited to participate, and the Portuguese edition of the Maslach Burnout Inventory - Human Services Survey (MBI-HSS) was applied, from March 25, 2021, to May 17, 2021. In terms of sociodemographic and workplace setting data, the participants were asked about their age, gender, marital status, the existence of dependent children, their workplace region (North, Centre, Lisbon and Tagus Valley, Alentejo, or Algarve), whether they had worked locally at the Public Health Unit of their primary healthcare clusters, or if they had been recruited to work at their Regional Health Departments or at the National Directorate-General of Health, where they would mainly serve functions regarding data processing, publication, and communication. We also asked whether the residents had worked at the office in the Public Health Units, or Regional and/or National Departments, or if they had worked from home (the National Epidemiological Surveillance System is one hundred per cent computerized and can be accessed anywhere on the Internet via authentication). Lastly, the participants were inquired about the periods of the pandemic peaks of COVID-19 incidence that had happened to date during which they had worked: the 1st peak in March/April 2020, the 2nd peak in October/November 2020, and/or the 3rd peak, during January/February 2021. Due to the small size of our sample and privacy concerns, we did not ask about the residents’ year of residency.
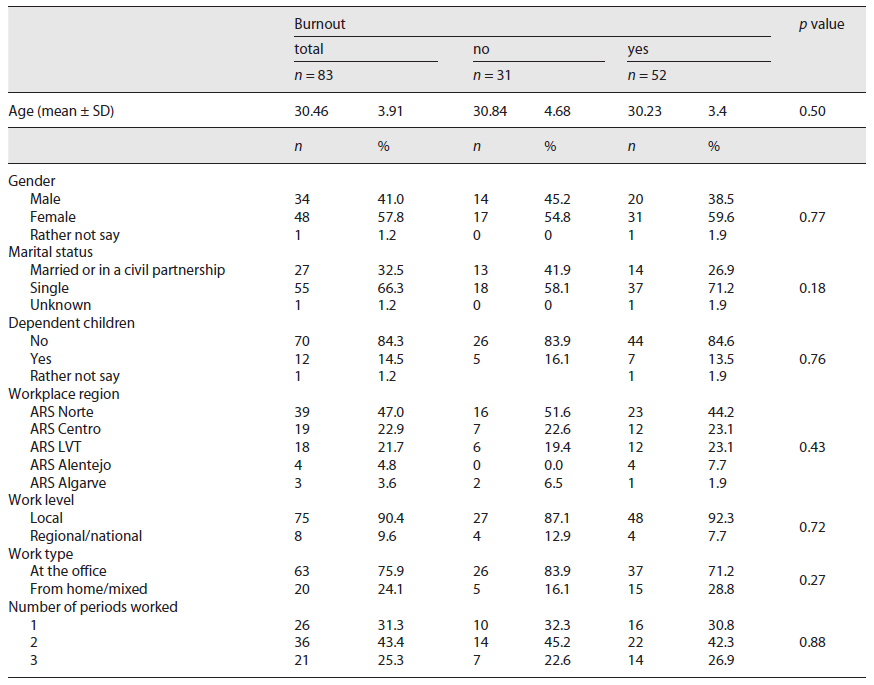
A total of 83 PHMRs participated. The majority were female (57.8%), had an average age of 30.46 (±3.91) years, and 66.3% were single. Most of the participants worked in the northern region (47%), at the local level (90.4%), and at the office (75.9%).
Informed consent was obtained by the Helsinki Declaration, and the data were anonymized via the Microsoft Forms® software. The confidentiality and anonymity of the participants were preserved.
Measures of Variables
The Portuguese version 53 of the MBI-HSS 17 - a burnout psychological assessment instrument that has been used in over 95% of research regarding this syndrome 54 - was used in our study. This version of the MBI-HSS includes 22 ordinal items reflecting three dimensions of burnout: EE, DP, and lack of PA. A seven-point ordinal response format was used, ranging from “0 - never” to “6 - everyday.” The points obtained on each question are added to obtain the final score on each dimension. Cronbach’s alpha coefficients obtained in the original study were 0.90 for EE, 0.79 for DP, and 0.71 for PA 17. Cronbach’s alpha coefficients obtained with our sample were 0.843 for EE, 0.755 for DP, and 0.761 for PA.
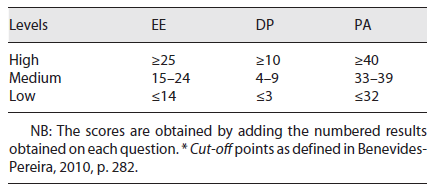
A person is said to be experiencing burnout if they simultaneously present high levels for the dimensions of EE and DP and low levels for the PA dimension 55. Regarding the cut-off points, we applied those suggested by Benevides-Pereira, 2008 56 (Table 1), also used in other studies with Portuguese health professionals 57, which are considered a valid alternative in countries with no validated cut-off points to extrapolate burnout levels from the frequency of symptoms (Table 1).
Models and Data Analysis Procedure
The collected data were processed using Microsoft Office Excel® 2017 and Statistical Package for Social Sciences (SPSS®), version 17.0. Categorical variables were presented as frequencies and percentages, and continuous variables as means and standard deviation (SD) for variables with skewed distributions. Pearson’s χ2 and independent samples t tests were used to evaluate the distributions of categorical and continuous variables, respectively, between the burnout and nonburnout groups, with a p value of 0.05 indicating statistical significance.
Results
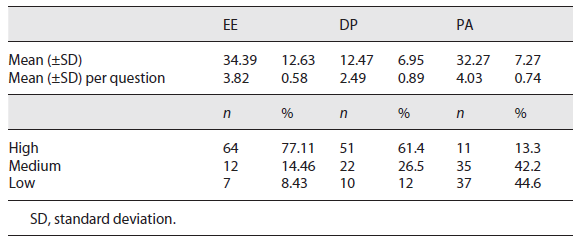
We considered high levels of EE and DP, and low levels of PA 56 (≥25 on EE, ≥10 on DP, and ≤32 on PA) as being altered levels of these dimensions 58. The maximum score for EE, DP, and PA is, respectively, 54, 30, and 48. Using the cut-off criteria defined by Benevides-Pereira 56 (see Table 1), we found that 77.11% of the participants had high levels of EE, 61.4% had high levels of DP, and 44.6% had low levels of PA (Table 2). The mean for the EE dimension was 34.39, with an SD of 12.63, the mean for the DP dimension was 12.47, with an SD of 6.95, and the mean for the PA dimension was 32.27, with an SD of 7.27. All these results can be consulted in Table 2.
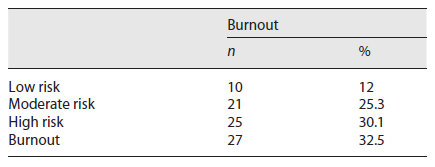
In what concerns burnout as a multidimensional construct it was defined, following Ebisui 58, as affecting an individual who was experiencing three altered dimensions. High risk for burnout was considered if the individual had two altered dimensions, moderate risk if they had one altered dimension, and low risk if they had no altered dimensions. Twenty-seven of the participants had altered levels in all three dimensions, twenty-five of them had altered levels in two dimensions, twenty-one had one altered dimension, and ten had no altered dimensions. Thus, 32.5% of the participants were burned out, 30.1% were at a high risk of developing burnout, 25.3% were at moderate risk, and 12% were at low risk (Table 3).
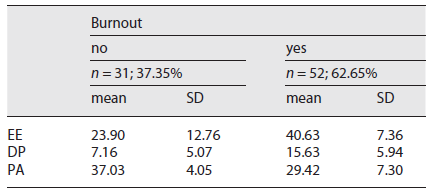
Following Pereira et al. 57, all burned-out professionals as well as those who had a high risk for developing this syndrome were considered to be experiencing burnout. Thus, comparing the participants with and with no burnout (Table 4), it was found that the professionals who were experiencing burnout (fifty-two of them, resulting from the addition of the twenty-seven that were burned out and the twenty-five that were at high risk) had high levels of EE (40.63 ± 7.36; mean ± SD) when compared to their not burned-out peers. Concerning the dimension of DP, the professionals who were experiencing burnout also showed high levels (15.63 ± 5.94; mean ± SD) when compared to professionals who were not experiencing burnout, whose levels of DP were moderate (7.16 ± 5.07; mean ± SD). Finally, it was found that professionals who were experiencing burnout had low levels of PA (29.42 ± 7.30; mean ± SD) (Table 4).
An independent sample t test (α = 0.05) was performed for age, and Pearson’s χ2 analyses were performed for the rest of the sociodemographic and work-related variables, to evaluate whether there was an association between them and the existence of burnout. No significant differences, however, were found. Thus, further analyses were deemed unnecessary (Table 5).
Discussion
The COVID-19 pandemic has brought a very high workload on the Portuguese PHMR. Hence, not surprisingly, the present study shows extreme levels on all the three components of burnout, as well as a high prevalence of the syndrome among this population.
The awareness these professionals have toward the issue of mental health, along with the proximity to the researchers - fellow residents - might explain the high response rate (about 42% of the total universe of Portuguese PHMR answered the questionnaire), when compared with similar studies on the same topic (24% on Lancee et al. 59 and 39% on Manzano García et al. 60, for instance). There may be, however, a selection bias, as we do not know the participants’ mental illness backgrounds. Respondents in a worse mental health state may have been more motivated to participate in the study. Conversely, the exact opposite can be true, as some of those who are already experiencing burnout may not have had the willpower to share their experience.
Another factor of note was the scores themselves, which seem to be exceptionally high. When looking at other studies on the same topic, we get confronted with much lower scores. Silva et al. 61 found in their sample that a mere 7% of participants showed high levels of EE, and a 2017 review of 1,406 health professionals by Parola et al. 16 found that 17.3% of them were experiencing burnout. A 2016 study by Marôco et al. 62 done on Portuguese nurses and doctors found higher values, with 43.6% of participants suffering from burnout, which, while expressive, is still far from the 62.6% obtained in the present study. However, when focusing our attention on similar studies done during the COVID-19 pandemic, we find results more on par with the ones obtained in the present study. A 2020 review by Amanullah and Ramesh Shankar. 63 reports that Giusti et al. 64, who surveyed 330 health professionals working in a health institution in Northern Italy using the MBI-HSS, found that more than two-thirds of participants had reported moderate to severe levels of EE and reduced PA, and more than a quarter of the sample reported moderate to severe levels of DP. These findings were corroborated by Dimitriu et al. 65, who, using the Maslach Burnout Inventory - Medical Personnel, surveyed 100 medical residents and, on average, 76% of the sample reported burnout. The authors also noted that this level of burnout was “superior to studies conducted in normal periods” 65.
As to what the sociodemographic data are concerned, the absence of any statistically significant differences among the different tiers can be an indicator of a de facto poor influence of these factors on such syndrome or, simply, that a sample of 83 individuals is of an insufficient size for it to be possible to detect how these data can be associated, as either risk or protective factors, with the burnout syndrome. A major limitation that this study has, however, has to do with the fact that no information was gathered regarding the characteristics of the work each PHMR had to do, and the conditions they had to work in. There is also no information regarding each participant’s mental health background, specifically on what concerns burnout syndrome. Therefore, to be able to design effective interventions to mitigate the burden this syndrome has, further studies need to address these two issues.
These results are, nevertheless, congruent with the increased workload that fell upon the PHMR during the pandemic, with little to no time left for adequate resting and other extra-work activities. The rising wave of new cases, despite the professionals’ best efforts, might have led to a sense of lack of control in the workplace, as well as frustration for knowing one was struggling against the tide. The lack of sufficient resources in the work setting could have exacerbated these feelings, contributing to disengagement, and aggravating the risk of burnout. This study suggests, therefore, that there is an urgent need for the reinforcement of Public Health Units’ resources, especially through the recruitment of more personnel. This way the workload in future pandemic situations can be mitigated and better managed.
Conclusion
The present study shows strong indicators that a considerable portion of the Portuguese PHMR exhibited high risk or was, indeed, experiencing burnout syndrome during the months of the COVID-19 pandemic. The study has, however, limitations. Further studies should be done to determine whether this phenomenon was specific to this period or if similar findings would come up during more normal times. The characteristics of the work and its conditions should also be assessed, so better clues for effective interventions may be obtained. A greater sample might also have shed light on putative protective and risk factors for burnout syndrome among this population.
Although some sociodemographic and work-related data were collected, several other putative preponderant factors were left out of the analysis, which could have contributed to a better more comprehensive approach to the problem. Further studies should also assess factors such as the ratio of professionals (doctors, nurses, environmental health technicians, and so on) per thousand people served by the local healthcare cluster the PHMR is working at, how the PHMR had felt their work demands had changed and how they felt it had influenced their health, and whether they felt they had sufficient material and human resources to meet the demands.
Overall, however, this study suggests that the Portuguese Public Health infrastructure is not adequately prepared to sustain the strain a global pandemic such as the SARS-CoV-2 imposes. We are dealing with cyclical events which are bound to be repeated. The information systems in existence proved insufficient to deal with the overflow of data and had to be optimized as the pandemic was progressing. This issue, therefore, should be addressed. The existent contingency plans also turned out to be inadequate to curb the impact of the crisis. Better contingency plans, which contemplate the creation of emergency teams of professionals (such as the military) that could be called upon when necessary and plans to better and more effectively communicate with the population should therefore be created.
Statement of Ethics
Participants informed written consent was obtained by the World Medical Association Declaration of Helsinki, before the participation in the study. The collected data were anonymized using the Microsoft Forms® software, and care was taken to exclude people whose geodemographic data might have allowed their identification among the participants. Those people were identified before answering the questionnaire and were not allowed to follow through. Confidentiality of the data and the anonymity of the participants were preserved.

