











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) responsible for coronavirus disease 2019 (COVID-19) was declared a pandemic in March 2020 1, and thus, lockdown measures have been widely used to control and prevent virus transmission in pandemic regions 2-3. COVID-19 was first reported in Morocco on March 2, 2020. The Moroccan authorities, for preventing the spread of the pandemic and preserving the health and safety of citizens, have decided to declare a “state of health emergency,” and as a crisis governance measure, a lockdown was imposed on the whole country from March 2 until 20 May 2020 4. Although the measures exhibited their effect on infection prevention and control worldwide 2, the widespread lockdown inevitably imposed psychological effects on populations 5, particularly anxiety 6.
Psychiatric disorders are often linked with chronic medical illness 7-8. In fact, the diagnosis of a chronic disease can affect self-confidence, reduce one’s quality of life 9, and cause uncertainty 10, anxiety symptoms, and depression symptoms 11, because the consequences of the new situation can disrupt the individual’s overall emotional balance 12. Hence, numerous reports have described emotional disturbances in adult celiac disease (CeD) 13-14. CeD is a chronic immune-mediated disorder triggered by the ingestion of gluten that appears in genetically predisposed patients 15. The name gluten is applied to a collective set of proteins for storage that are found in grains of wheat, barley, and rye 16. The disease occurs in adults and children at rates approaching 1% of the population in many countries 17.
In fact, ingestion of these foods causes serious and permanent damage that can lead to the atrophy of the small intestine villi if the disorder is not diagnosed quickly, and adequate therapy did not start 18. Consequently, the main treatment for CeD is lifelong adherence to a gluten-free diet (GFD) 17. Following a GFD not only helps reverse intestinal injury, normalize nutrient absorption, and relieve symptoms 19 but also reduces the risk of serious future complications, including osteoporosis, malignancy, and fertility difficulties 20.
CeD has been associated with certain infections in previous studies 19-20, like an increased risk of hospital admission for influenza 21 and of community-acquired pneumonia in CeD-unvaccinated subjects compared to controls. Recently, immune-mediated gastrointestinal diseases have been associated with SARS-CoV-2 infection and its complications 22-23.
Being at high risk of infection in addition to emotional disturbances by the concomitant presence of chronic disease 13-24, CeD patients may suffer from anxiety or increase this condition 9-24, because of the COVID-19 widespread lockdown. Moreover, CeD patients might also fear the lack of gluten-free food 24. Accordingly, this study aimed to assess COVID-19-related anxiety in a sample of adults with CeD in comparison with a matched healthy group.
Methods
Population and Data Collection
In this cross-sectional study, conducted between April 15 and May 15, 2020, we invited CeD patients and a matched healthy group to complete a web-based COVID-19 and related lockdown anxiety survey. We received 103 and 101 responses (from CeD patients and the comparison group, respectively), matching our inclusion criteria. Exclusion criteria for CeD patients were the presence of other diseases or disorders than CeD, consumption of psychotropic drugs, and secondary causes of villous atrophy. Consequently, participants were Moroccan adults, aged between 18 and 59 years, those with CeD were diagnosed according to international criteria 25 and followed a GFD, while the comparison group consisted of healthy asymptomatic individuals, not diagnosed, or treated for any disease and not pursuing a specific diet. The questionnaire was administered online after participants filled out consent for the collection, handling, and storage of data, which were included in the presentation of the questionnaire. The average time to complete the protocol was approximately 15 min.
General Information
Data about demographic and clinical features, including gender, age, area of residence (urban or rural), age of CeD diagnosis, and severity perception of the disease (on a scale of 0 to 10 with 0 being not severe at all and 10 extremely severe), and adherence to GFD for CeD participants were recorded.
COVID-19 and Related Lockdown Questionnaire
The web survey included 13 multiple-choice questions aiming to evaluate the perception of the COVID-19 pandemic and related lockdowns. We asked if participants are worried about contracting the disease, if their sleep and physical activity are compromised because of the lockdown, if the CeD patients believe they are at an increased risk of contracting COVID-19 when compared to the general population, and if they are worried about their health with the postponed medical consulting. We also asked participants whether they are worried about the possible shortage of food in general and of gluten-free products for CeD participants, and whether this affected their adherence to the GFD.
Anxiety Measure
Anxiety was assessed with the State and Trait Anxiety Inventory (STAI test), made up of 2 axes (Y1 for state anxiety and Y2 for trait anxiety), both consisting of 20 multiple-choice items; each item has a score from 1 to 4 so that the total score of the two axes can range from 20 to 80 26. The State Anxiety Scale, State-Trait Anxiety Inventory 1 (STAI-Y1) (S-Anxiety), evaluates the current state of anxiety, asking how respondents feel “right now,” using items that measure subjective feelings of apprehension, tension, nervousness, worry, and activation/arousal of the autonomic nervous system. The Trait Anxiety Scale, State-Trait Anxiety Inventory 2 (STAI-Y2) (T-Anxiety), evaluates relatively stable aspects of “anxiety proneness,” including general states of calmness, confidence, and security 27. This test was selected on the basis of its simplicity, validity, and reliability 26, and also because it was used in studies evaluating anxiety and distinguishing “state” anxiety from “trait” anxiety in patients with gastrointestinal diseases 28,29,30. The subjects evaluated were grouped as not anxious, anxious, and high anxious, according to Spielberger et al. 26 and Weinstein 31.
Statistical Analysis
Continuous variables were presented as means with standard deviations and proportions for categorical variables. Numerical variables were analyzed using the Student t test. The χ2 test was used to assess statistical significance between qualitative variables.
Relations between study variables were evaluated using bivariate analysis with Pearson or Spearman (rho) coefficient for skewed data with a two-tailed p < 0.05 indicating statistical significance. Statistical analysis was performed using Statistical Package for Social Sciences (version 19.0, SPSS, Inc.) software.
Results
First, we displayed the sociodemographic and clinical characteristics of the participants (Table 1). The majority were resident in an urban area (88.3% of CeD patients and 86.1% of the comparison group) and were women (77.7% of CeD patients and 66.3% of the comparison group), and their mean age at the time of the survey was 29.01 ± 8.46 years for CeD participants (ranging from 18 to 55 years old) and 29.30 ± 8.92 for comparison group members (ranging from 18 to 59 years old). We found no differences in sex, age, and residence between the two groups.
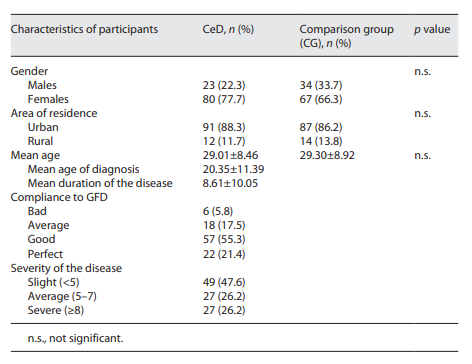
The mean age of diagnosis of CeD in our sample was 20.35 ± 11.39 years with extremes going from 1 to 50 years, the mean duration of the disease was 8.61 ± 10.05 years ranging from 3 months to 41 years, and the personal reported compliance to GFD was mostly good. The mean score of the severity perception of the disease on a scale of ten was 5.09 ± 3.02 with extremes ranging from 0 to 10 and with a percentage of 12.5% of CeD participants perceiving the severity of their disease at its highest (score 10).
In our study, data analysis revealed, according to the index of internal consistency, that both STAI test scales had a good reliability (Cronbach alpha = 0.91 for STAI-Y1 and Cronbach alpha = 0.88 for STAI-Y2). The evaluation of anxiety (Table 2) revealed that state anxiety (Y1) was present among 65.3% of CeD and 41.6% of comparison group members (χ2 = 11.02; p < 0.001).
Table 2 State and trait anxiety among CeD and healthy participants and relative statistical comparison (p)
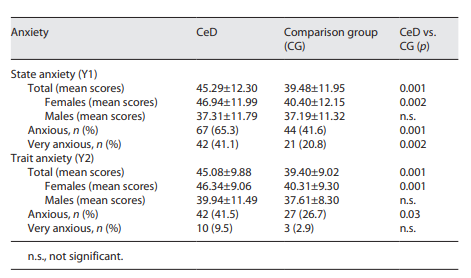
The mean score in the state anxiety test (Y1) among CeD participants was higher than among the comparison group (45.29 ± 12 vs. 39.48 ±11.94) (t = 3.35; p < 0.001). By gender, CeD women had higher state anxiety mean score than the comparison group (t = 3.23; p = 0.002), while no significant difference was reported among males in the two groups (t = 0.30; p = 0.76) (Table 2).
Furthermore, very high state anxiety scores (defined as scores >55 for women and scores >48 for males) were found among CeD patients more than among controls (41.1% vs. 20.8%) (χ2 = 9.46; p = 0.002). The STAI-Y2 exploring trait anxiety showed that 41.5% of CeD participants were having anxiety as a trait against 26.7% of controls (Table 2) (χ2 = 4.73; p = 0.03).
CeD group had a significantly higher mean score at STAI-Y2 than the comparison group (45.08 ± 9.88 and 39.40 ± 9.02, respectively) (t = 4.15; p < 0.001), and similar to state anxiety, CeD women had higher mean score on STAI-Y2 than their compatriots on the comparison group (t = 2.32; p < 0.001). Very high trait anxiety scores (defined as >61 for women and scores >51 for males) were reported among 9.50% of CeDs against 2.97% of the comparison group (χ2 = 3.60; p > 0.05).
Interestingly, trait anxiety was present among participants diagnosed with CeD for a mean period of 6.27 years, while the ones having no trait anxiety were diagnosed for more than 10 years (t = 2.07; p = 0.04). Also, we found an association between age and state anxiety scores, as older participants had higher state anxiety scores while for anxiety as a trait, scores decreased with age declaring more trait anxiety among younger participants.
The findings of the web survey in relation to the COVID-19 pandemic and related lockdown reported no significant differences between the CeD group and the comparison group concerning the respect for confinement (79.4% and 85.1%, respectively) and perceived life conditions (normal in 53.9% and 61.4% of cases and difficult in 24.5% and 18.8% of cases, respectively). Among the CeD group, the respect for confinement was associated with high perceived severity of the disease (χ2 = 12.127; p < 0.02), and also were the difficult life conditions associated with the urban origin of participants (χ2 = 6.57; p < 0.03).
Concerning participant worries about contamination, consequences of the pandemic, and the lockdown, and CeD group generally expressed more worries than the comparison group (Table 3). Thus, among the CeD group, the worries about shortness in gluten-free products were associated with high perceived severity of the disease (χ2 = 13.23; p < 0.04) and the worries about the professional stability were associated with the urban origin of the participants (χ2 = 8.98; p < 0.02). Sleep was also more affected among CeD participants than controls (χ2 = 11.45; p = 0.01) and women were more affected than men (χ2 = 10.50; p < 0.01). The preoccupations about health related to postponed medical consulting were more expressed among CeD than controls (χ2 = 11.66; p = 0.009).
Table 3 Perceived COVID-19 pandemic and effects on state anxiety among CeD patients and comparison group
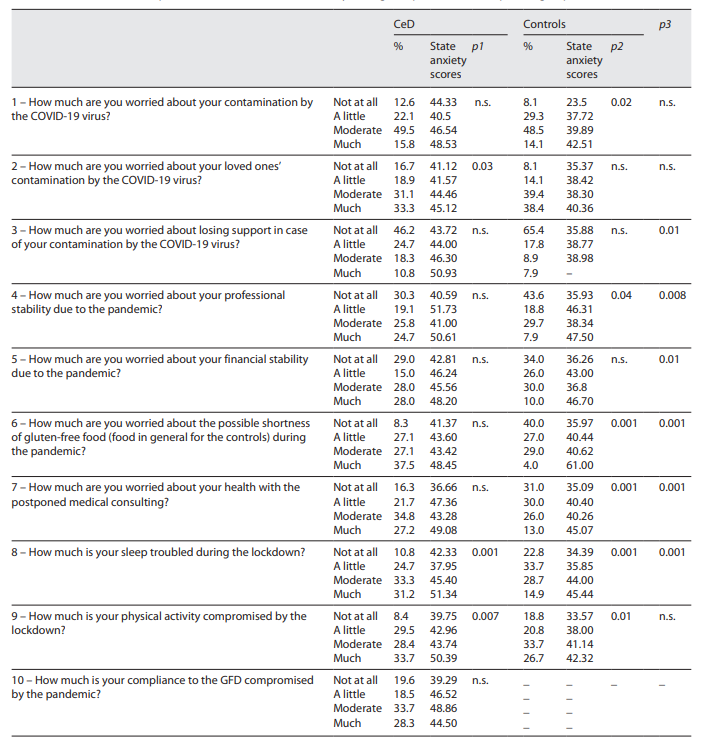
The analysis of the effect of the COVID-19 pandemic and related lockdown on state anxiety among CeD patients in comparison with members of the comparison group showed in addition to what is reported in Table 3 a significant correlation between difficult life conditions and state anxiety in both CeD patients (r = 0.29; p = 0.004) and controls (r = 0.43; p < 0.001), between high scores at STAI-Y1 and high perceived severity of the disease among CeD group (r = 0.24; p = 0.007), as well as between good compliance to GFD and less state anxiety (r = 0.31; p = 0.002). To the question “do you think that you are at higher risk of coronavirus 19 infection because you have CeD?” 61.8% of CeD participants (mostly women) thought they were (χ2 = 7.66; p < 0.006). The participants who thought they were at higher risk of contamination had significantly higher state anxiety mean scores than their compatriots who did not express these thoughts (t = 2.93; p = 0.004). While as a response to the question “do you think you are at lower risk of coronavirus 19 infection because you do not suffer from a chronic disease?” 62.4% of controls thought they were not, with no difference between the two genders and no significant association with state anxiety (t = 0.17; p = 0.87).
Discussion
In this first study on the effect of COVID-19 pandemic and related lockdown on CeD patients compared to the normal population from Morocco, we found that this critical situation had a deep influence on CeD patients. One of the findings of our study was the presence of state anxiety among 65.3% of CeD and 41.6% of the comparison group. The mean scores in the state anxiety test (Y1) among CeD participants were higher than among controls (45.29 ± 12 vs. 39.48 ± 11.94) and women were more affected than men. Although this may be due to the high number of women in the study sample, the number of men in the sample is still representative (around 25%) which could reflect a gender difference in anxiety 32.
In fact, state anxiety expresses the psychological and physiological transient reactions that are directly related to adverse conditions at a certain moment 27. During the current COVID-19 pandemic and related lockdown, limitations to free moving, uncertainty, and fear of facing the advances of viral infections, lack of physical activity, technological capacities required to access food, remote working, and confinement are fundamental factors shaping the mental health deterioration of the general population during the pandemic 33. Kontoangelos et al. 34 reviewed the psychological effects of the COVID-19 pandemic and described that children, older people, and those with underlying health conditions are likely to feel worried, anxious, and fearful, which can be extremely frightening.
In the same spirit, in a recent study conducted among a group of Turkish CeDs, patients’ state anxiety index was 40.7 ± 7.9, based on the STAI scale, and all patients were evaluated as mildly anxious 35. The greater worry in older people and females in our study is in line with a recent Chinese study 36. The study reported that the female gender is associated with a greater psychological impact of the outbreak and higher levels of stress, anxiety, and depression 36. In the same spirit, another study also reported that the COVID-19 pandemic has impacted a proportion of patients with CeD, in particular, women and older people 24.
The other relevant finding in our study was that anxiety as a trait was present among 41.5% of CeD participants against 26.7% of controls and that the difference between the two groups was statistically significant. Conversely to state anxiety, the term trait anxiety refers to a personality trait and describes individual differences related to a propensity toward current state anxiety. Therefore, trait anxiety is comparatively stable over time, and it is considered to be a significant characteristic of patients with anxiety disorders because they have higher persistent anxiety than healthy individuals 27.
Our results are joining several studies that have demonstrated the presence of anxiety and depression in people with CeD 12-37. A recent systematic review and meta-analysis assessing celiac patients in nonpandemic conditions 38 reported anxiety (OR 6.03, 95% CI: 2.22-16.35; p < 0.0001) was higher in celiac patients compared with the general population. Associations between depression and anxiety are apparent as a result of the psychological and social implications of CeD comprising social isolation, avoiding going out because of the risk of contamination, having to always declare the condition among friends and colleagues, and having to explain the diagnosis of CD as opposed to a life choice of GFD, etc. 14-39.
In our study, we also reported that good compliance to GFD was correlated with less state anxiety. This was in line with previous studies affirming that adherence to GFD correlates with lower anxiety 12 and that associations between mental health indicators and adherence to GFD were strong 40. An Italian study also demonstrated that the improving psychological well-being of patients was associated with improved self-reported adherence to GFD 41. In fact, adherence to a GFD is largely accepted to be challenging; it requires motivation, knowledge, and modification of behaviors. GF dietary adherence can be influenced by many factors including symptoms of ingestion of gluten, knowledge of GF foods, understanding of food labels, cost and availability of GF foods, and membership in a coeliac society 41.
Another result depicted in the present investigation revealed that 61.8% of participants thought they were at higher risk of contracting COVID-19 infection as they had CeD. The participants who thought they were at higher risk of contamination had significantly higher state anxiety mean scores than their compatriots who did not express these thoughts. This result is in contrast with the results of Siniscalchi et al. 24 who found that the majority of respondents to their study did not report feeling more vulnerable to COVID-19 due to their CeD. This discrepancy may be explained by the lack of medical advice and sharing of scientific updates in our context the opposite of the cited study that implemented the use of telemedicine.
In fact, there is still doubt whether the presence of any immunological disorder is a risk factor for COVID-19. A large study performed with 10,737 CeD patients from Argentina, Australia, Canada, Italy, Mexico, New Zealand, Spain, Uruguay, and the USA during the pandemic showed that CeD patients have similar chances of contracting SARS-CoV-2, and it is unnecessary to take additional care to prevent exposure aside from the recommendations to the general population 42. In addition, a cohort study conducted in Sweden with 40,963 CeD individuals showed that they were neither at increased risk of hospitalization for COVID-19 than the control ones nor at high risk for severe disease outcomes and mortality 43.
Limitations
Our study involves only a few number of patients; however, it should be kept in mind that diagnosed CeD is not a very common disorder and thus the possibility to have a high number of patients can be reached only in the case of large multicenter studies. The small number of patients involved in our study did not allow us to analyze data on state anxiety controlling for trait anxiety and thus better attribute anxiety in celiac patients to the situation experienced during the pandemic. Also, the sample of this study, as other ones realized among CeD patients, is formed mainly by women, making it difficult to explain whether sex is a relevant variable in the analysis and also the female predominance of systemic autoimmune diseases might accentuate this difficulty.
Conclusion
The results of this survey allow a better understanding of the health-related pandemic effects on people with the CeD living in Morocco. It demonstrates that COVID-19 and related lockdowns had a serious impact on the psychological balance of these patients by increasing their state of anxiety. It also indicates that trait anxiety is critically present among CeD patients. The survey results underlined the need to encourage the psychological care of CeD patients in order to help manage their anxiety in addition to considering remote medical visits during this ongoing pandemic to provide mental health support.
Statement of Ethics
Written approval was obtained from the Sultan Moulay Slimane University before the initiation of this study with the number of FST/LGB/2020/15; MAR.2020-SEPT.2020. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants. All data were confidential and protected at all stages of the study.
Funding Sources
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Contributions
Boutahar Kaltoum: participation in the design of the study, analysis and interpretation of the data, and writing of the article. Ihbour Said: participation in the design of the study, analysis and interpretation of the data, and contribution to the writing of the article. Hadi Karima: obtaining the data, participating in the interpretation of the results, and reviewing the content of the article. Kaoutar Kamal: obtaining data and reviewing the content of the article. Chetoui Ahmed and El Kardoudi Abdslam: obtaining data and reviewing the content of the article. Najimi Mohamed and Chigr Fatiha: design of the study protocol and critical review of the intellectual content of the article.

