











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Vaccine hesitancy (VH) is a widespread phenomenon across the Globe that might put at risk the health and well-being of populations, representing a considerable challenge for healthcare professionals. VH has been defined as the delay or refusal of vaccines despite its availability 1. The World Health Organisation recently proposed that VH should be considered as a “motivational state of being conflicted about, or opposed to, getting vaccinated; includes intentions and willingness” 2 (p. ii). While VH has been represented as a behaviour, it is a psychological state 3. VH is context-specific, varying according to time and place, as well as with the types of vaccines 1. Even though the complexity of VH, research shows that distrust in science and medicine is a critical factor 4-6. Therefore, interaction between healthcare professionals and parents is key for enhancing trust 7,8. Indeed, healthcare professionals are considered to be the most consistent and reliable source of vaccine information among parents 9. There is evidence that even in cases of initial positions of vaccine delay or refusal, trustful communication with healthcare professionals can influence parents’ decisions regarding vaccine adherence 10. Hence, poor communication by healthcare professionals is highly detrimental to the interaction with parents, contributing to the increase of their doubts and concerns regarding the immunization of their children 11. Research, to date, suggests the need for healthcare professionals to adapt their communication style to the needs and characteristics of parents when discussing childhood vaccination 12. The participative format style of communication, which is based on a patient-centred approach, has been found to be the most fruitful in cases of VH, contributing to the establishment of a long-lasting relationship of trust. This style of communication includes effective communication practices for healthcare professionals to adopt when discussing children’s immunization with parents, such as: openly discussing the need for vaccination, showing respect and empathy regarding parents’ concerns and doubts, adopting a screening tool to identify parents’ concerns and address them with tailored information 13.
Among the evidence-based methods developed for healthcare providers to use when discussing vaccination with parents, motivational interviewing (MI) emerges as a collaborative counselling style that aims to elicit a person’s motivation to take action on a particular health issue 14. As a communication style, rather than a strategy 14,15, the MI aims to shape the routine practice of clinicians to catalyse patients’ intrinsic motivation to change in terms of health behaviour - in this case, to intervene with parents holding varying degrees of indecision towards specific vaccines or vaccination in general 14,16,17. The MI method is part of a broad spectrum of models for communicating with patients who display VH 18. That is the case with the A.S.K. approach or the C.A.S.E. framework, which provides a guide for answering patients’ questions and concerns, providing clinical evidence that healthcare professionals can present 19. Thus, both models consist of an information deficit model, i.e., based on providing information on immunization issues, by explaining the benefits and risks of vaccination. However, the effectiveness of this approach raises reservations 19. Moreover, these models also favour one-way communication rather than a professional-patient interaction, which, from a patient-centred perspective, is designed to give the patient greater latitude in decision-making processes 14,15. In turn, frameworks such as MI or Behaviour Change Counselling (BCC) emerge precisely within the range of approaches aimed at greater involvement and dialogue between patients and health professionals 19. In the case of MI, it differs from the previous frameworks in the sense that it departs from the conventional counselling model, favouring a more symmetrical relationship based on three central characteristics that define its spirit: (i) collaborative, aiming at cooperation and active, shared conversation and co-decision making, as opposed to an unequal power relationship in which the expert clinician directs a passive patient; (ii) evocative, in the sense of evoking patients’ values, concerns and arguments, in order to activate their own motivation and resources for change; and (iii) honouring patient autonomy, in which clinicians may inform, advise - and even warn - patients, but ultimately accept their decision 14. Expressing these characteristics, MI relies on a fundamental set of basic skills aimed at encouraging patients’ ability to express their doubts and concerns: open-ended questioning, affirming, reflective listening, and summarizing - often abbreviated to OARS 17,20. MI has been successfully used in situations of VH regarding newborn immunization 21, HPV vaccine e.g., 22-23, and vaccine against the flu 24. There is evidence that healthcare professionals’ training on MI increased their self-efficacy when approaching vaccine-hesitant parents 23,25. MI training is generally developed in in-person sessions, including an initial exposition of the theory and principles of MI, followed by the active participation of trainees in immunization-specific simulation exercises. At the end of the training, trainees are asked to reflect on and share with their peers about the main challenges they face when dealing with vaccine-hesitant parents 26.
In recent decades, research on MI has largely been conducted outside the field of immunization 20-27. Initially developed in the context of alcohol abuse, its application has been progressively extended to other clinical settings, such as intervention on addiction, lifestyle, mental health, and chronic diseases 19,20, 27‒32. In the field of immunization, different studies measure the effectiveness of MI training by resorting to vaccination coverage rates as the sole outcome 24,33-36. Other published research mobilizes tools to measure the impact of MI training in terms of health professionals’ capacity to acknowledge and put into practice its principles - combining or not with other outcomes to measure the effectiveness of MI training on VH (e.g., vaccination rates, patients declared intentions to get vaccinated, etc.). Namely, trainees’ MI competencies can be quantified and measured through various integrity and fidelity coding systems, such as the Motivational Interviewing Skills Code (MISC), the Motivational Interviewing Treatment Integrity (MITI) scale, the Independent Tape Rater Scale (ITRS), or the Motivational Interviewing Knowledge and Attitude Test (MIKAT) 25,29,37,38. These validated standardized measures (consisting of dimensions/constructs and items to measure them) can be incorporated into various pre-post methodological designs and applied to health professionals in different ways. This is the case with self-completion surveys 38 or observation techniques, either through the standardized patient technique - i.e., consultation with a role-playing patient showing ambivalence about changing health-related behaviour - or in the context of a medical consultation with real patients 37. Other studies have also developed more elaborated methodological models to measure the impact of MI training, relying on randomized trials 22,23,39, which allow for a comparison of skills acquired between a group of MI trainees (intervention group) and untrained participants (control group). In these different methodological protocols for measuring training and evaluating its effectiveness in addressing VH, the results present significant increases in clinicians’ MI competencies, albeit with exceptions and nuances relevant to highlight.
Data from the XXX project show that MI is not a generalized practice among healthcare professionals in Portugal. Indeed, vaccine-hesitant parents have often described that healthcare professionals usually employ a paternalistic model of communication adopting an authoritarian and directive discourse tone 6. Concerning immunization rates in children, Portuguese parents are the most vaccine-confident compared to parents from other European countries 6,40 - a tendency that extends to the COVID-19 vaccine coverage 41. However, given the documented phenomena of vaccine refusal at marginal levels 42-44, outbreaks of these vaccine-preventable diseases are likely to resurface as a result of under-vaccinated or unvaccinated communities, as illustrated by two measles outbreaks occurred in this country in 2017 45,46. These findings stress the need for early intervention, namely by empowering healthcare professionals with immunization-specific communication skills to effectively address VH. The current study intends to assess the attainment of MI competencies by healthcare professionals in Portugal who may interact with vaccine-hesitant parents.
Materials and Methods
Overview of the Training Session
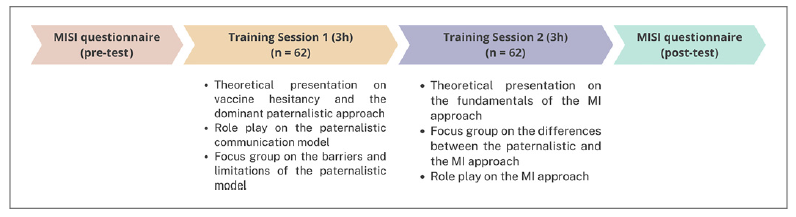
Educational training sessions on MI were conducted with healthcare professionals in Portugal to improve their communication skills in their interaction with vaccine-hesitant parents. The training was delivered in person by a sociologist and a social psychologist with previous training on immunization-specific MI. Activities were developed in two educational sessions, each one with a duration of 3 h, for a total of 6 h. In the first session, participants were provided with information on VH based on previous findings from the XXX project. A special focus was placed on the prevailing paternalistic communication model and its unsuitability in the context of VH. Following the theoretical presentation, three voluntary participants were asked to perform a play based on a cartoon depicting the interaction between a nurse and a couple with a baby in a vaccination setting where the paternalistic communication model was used 47. This activity was followed by a focus-group discussion about the main barriers to the interaction. In the second session, participants were presented with the fundamentals of the MI approach and its applicability to address parents’ concerns about their children immunization. After that, participants were provided with a cartoon depicting the same vaccination encounter as in the first session but, this time, the MI approach was used rather than the paternalistic one. The reading of this story was followed by a focus group about the main differences between the paternalistic model of communication and the MI approach. Finally, participants were divided into small groups, and they were asked to role-play using the MI approach based on a script of possible situations of VH and a brochure with written information about MI skills. The assessment of the training followed a pretest-post-test design as participants were asked to fill out the Motivational Interviewing Skills in Immunisation (MISI) questionnaire 25 at the beginning of the first session and at the end of the second one. The application of this written evaluation tool allowed us to assess participants’ MI knowledge and skills before and after the training took place. The following flowchart (Fig. 1) systematises the described MI training and assessment protocol.
MISI Questionnaire
The MISI-Motivational Interviewing Skills in Immunisation was developed as a protocol more suitable for large groups of participants, without the complexity and administration costs of other systems 25. By using this tool to assess skills in line with the spirit of MI, the results of this study can therefore be directly compared with those obtained in other research works using this system to measure the impact of MI training in healthcare professionals - nurses 25 and general practitioners 48. The MISI questionnaire consists of three core aspects of MI learning. Each core aspect is measured by a specific set of items, built on different types of variables: (i) MI Knowledge acquisition, is based on 6 items, all of which are nominal variables (with the number of response categories ranging from 3 to 6); (ii) MI skills application, one item is an open-ended question, in which the respondent writes a dialogue simulating an MI, starting from a hypothetical abstract situation of a parent expressing hesitation about vaccinating their child. A second set of items consists of 15 variables with a 6-point Likert scale to measure behaviours/attitudes consistent with MI skills; (iii) self-confidence in applying MI knowledge and skills in their routine clinical practice. A total of 7 items measure it, all of which are 10-point Likert scale variables.
The MISI questionnaire was validated by a panel of international MI experts and has shown good psychometric properties, namely internal consistency and reliability 25. To verify whether the several items measure the respective general construct, the internal consistency of the domains was analysed using the Kuder-Richardson coefficient (KR20) and Cronbach’s α for dichotomous and continuous variables, respectively. Specifically, in the case of the constructs MI Skills application and Confidence in using MI, internal consistency tests led to removing items with low correlation until the desired level of consistency was reached 25. As for the MI Knowledge dimension, the authors used the test-retest reliability (based on the intraclass correlation coefficient) to assess the accuracy of this construct across time - i.e., before and after the training sessions1 25.
In the case of the present study, Cronbach’s α for the set of items that compose the confidence dimension was 0.88 in the pre-training and 0.86 in the post-training, corresponding to a good consistency 48. In the MI skills dimension, the KR20 coefficient was set at 0.65 in the pretest and 0.79 in the post-test, indicating a questionable and acceptable internal consistency level, respectively. Finally, in MI knowledge, the Interclass Correlation Coefficient (ICC) was 0.551, representing a fair level of measurement reliability over time 49.
Ethics
Ethical approval for this study was obtained from the Instituto de Ciências Sociais, Universidade de Lisboa - host research centre of the XXX project in Portugal. At the beginning of the first session, participants were provided with information about the training, and they were asked to sign an informed consent form.
Sample
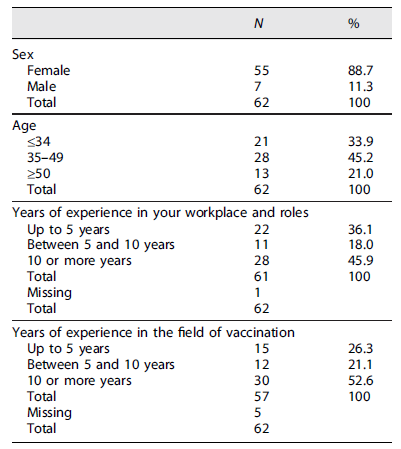
The study involved a total of 62 respondents: healthcare professionals (nurses and physicians) involved in the vaccination working on healthcare centres or in a public hospital and master students of community nursing who are already working as healthcare professionals. Most participants were female (88.7%). In addition, most respondents were aged between 35 and 49 years (45.2%), while approximately one-third of respondents were under 35 years old. Twenty-one per cent were 50 or over. Regarding the contexts of professional activity, almost half of the participants have more than a decade of professional experience in their current workplace (45.9%). In turn, 36.1% have a total experience of no more than 5 years - twice that of those with between 5 and 10 years (18%). Moreover, there is a prevalence of respondents whose direct professional contact with the field of vaccination extends to 10 years or more (52.6%). Approximately a quarter of the sample presents a professional trajectory in this medical domain that amounts to a maximum of 5 years (26.3%), followed by 21.1% between 5 and 10 years. The characterization of participants in the training can be found in Table 1.
Data Analysis
In terms of data coding, the MISI survey includes a scoring protocol. Apart from the treatment of the open-ended response, which follows a specific coding manual, the remaining items with closed-ended questions are subjected to a scoring system 25. For MI Knowledge, which consisted of 6 items, all multiple-response questions were transformed into dichotomous variables. For each question, one point was awarded for each correct answer category (i.e., category indicating MI-compliant knowledge) and 0 points for selecting the remaining options. A 6-point maximum could be achieved in this dimension. In the MI skills dimension, for items expressing MI-compliant behaviour, the two highest points on the 6-point Likert scale (frequently and extremely frequent categories) were assigned 1 point; for the items expressing non-compliant attitudes, only the choice of a category related to the lowest point of the scale (never) corresponds to 1 point attributed. The maximum score is, therefore, 15 points. As for the MI confidence dimension, the 10-point Likert scale is applied directly in the scoring system for each of the six items. The higher the value selected on the scale of each item, the higher the score awarded. Thus, 60 points is the upper limit for this dimension.
Finally, the number of points in each dimension is then converted linearly to a scale of 0-100, weighting the number of missing values (i.e., dividing the score by the number of items answered and multiplying by 100). Therefore, the final scores obtained in each section proportionally represent the level of the MI-convergent competencies demonstrated by the respondent in each dimension - i.e., MI knowledge, skills, and self-confidence - that the various items are intended to measure.
For data analysis, each dimension is subject to statistical procedures for comparing the scores between the two administration moments of the MISI survey, i.e., before and after the training sessions. Thus, in addition to descriptive statistics (having the mean as the privileged measure), the paired samples t test was the statistical procedure used to identify statistically significant differences between the two stages. This procedure includes the Cohen’s d effect size test to determine the magnitude of the effect of the training session on the three MI dimensions. This test makes it possible to quantify and qualify the impact of the training on the variation of scores per respondent: values around 0.2 express a small effect size; about 0.5, a moderate effect; around 0.8, a large effect; and very large if equal to or greater than 1.30 50,51. In addition, nonparametric Wilcoxon-Pratt tests for paired samples were used to compare the variation in scores between pre- and post-training sessions, differentiating respondents according to sociodemographic variables. Nonparametric tests were the most appropriate procedure due to the small size and imbalanced dimension between subgroups. Namely, statistically significant differences were tested according to the variables of years of experience in the workplace and years of experience in the field of vaccination. All statistical operations were performed using the SPSS software (version 29).
Results
Analysing the mean scores obtained in the three parameters for assessing MI competencies, there is an increase in the average points on all dimensions between the two temporal points - i.e., before and after the training (see Fig. 2). Indeed, while the hierarchy of scores maintains, is noticeable the inflation in the mean scores between the pre- and post-training session stages. The largest increase in the average score is observed on the dimension of sense of confidence, with an increment of approximately 18 points. In the remaining two dimensions, Perception of Skills and Acquisition of Knowledge, the variation between stages is similar: a rise of nearly 12 points in both cases.
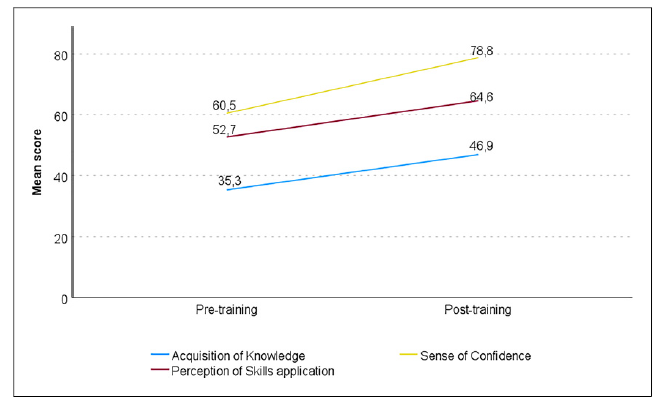
Fig. 2 Mean scores before and after the training session by dimension of the MISI survey (own calculations).
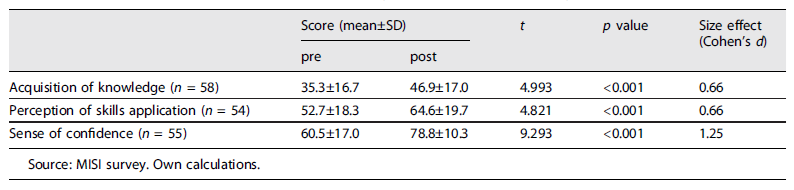
To assess whether the differences in the mean scores between the two moments for measuring knowledge and skills are statistically significant, a paired samples t test was performed (see Table 2). In addition to significant differences in the three dimensions of the survey, no effect size is qualifiable as weak 50. Sense of confidence in resorting to MI stands out, presenting a very large effect (t(54) = 9.293; p < 0.001; d = 1.25), followed by acquisition of knowledge (t(57) = 4.993; p < 0.001; d = 0.66), and perception of skills application (t(53) = 4.821; p < 0.001; d = 0.66), both with a medium effect. Thus, it is on the scale for measuring participants’ perceptions of self-confidence to apply MI knowledge and skills in their daily practice that the impact of the training is revealed to be higher. This result converges with prior studies 48, whereas, in the precursor research, MI-knowledge registered the largest effect size 25. No sufficient data were obtained to analyse the open-ended response regarding the application of MI skills. In this question, a situational exercise was presented and participants were asked to imagine and write a real-life dialogue with a vaccine-hesitant parent. The coding guide presents the scores to be attributed to each MI skills written by participants in the imagined dialogue, such as open-ended questions, reflective-listening and affirmative statements. However, most participants skipped this question or gave very brief answers, not including a dialogue that can be evaluated using the pre-defined criteria.
Table 2 Mean scores before and after the training session, by dimension of the MISI survey (T test and Cohen’s effect size)
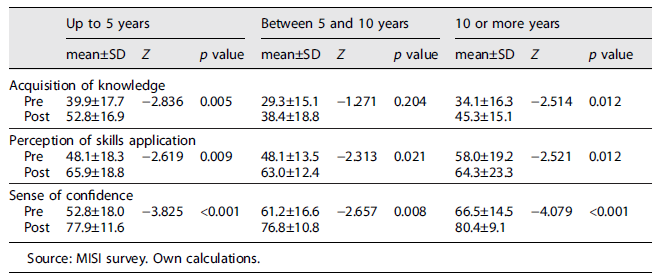
Additional comparative analyses were carried out to obtain a better understanding of the variations in the mean scores. In particular, the focus was on the sociodemographic variables related to the context of the participants’ professional activity resorting to Wilcoxon-Pratt tests. Firstly, there are significant differences in all parameters across the different groups according to years of experience in the respective workplace (see Table 3). The exception rests among respondents between 5 and 10 years, where the variation in the mean score before and after the training in MI is not significant for the dimension of acquisition of knowledge (Z = −1.271; p = 0.204).
Table 3 Mean scores of participants, by dimension of the MISI survey, by years of experience in the workplace
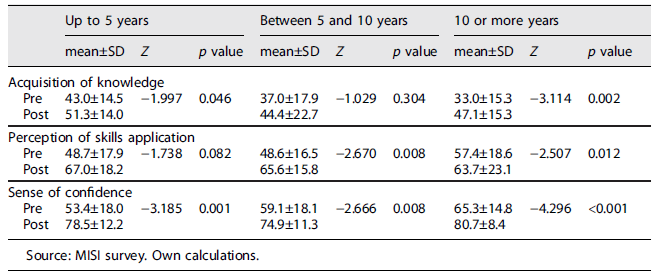
A more composite scenario is found when analysing the score distribution of respondents according to the years of professional experience in the field of vaccination (see Table 4). In this case, it is only among respondents with ten or more years of experience that significant differences are present in all dimensions. In addition, for participants with fewer years of experience (category up to 5 years), it is only in perception of skills application that there is no significant difference between the average evaluation made before and after the training (Z = −1.738; p = 0.082). As for respondents with 5-10 years of experience, it is in the dimension related to knowledge in the more theoretical component, acquisition of knowledge (Z = −1.029; p = 0.304), that no significant variation occurs. To that extent, if the significant oscillation in the sense of confidence is transversal across all groups, significant differences in the perception of practical MI skills acquired are limited to the segments that aggregate participants with higher years of experience - i.e., between 5 and 10 years and 10 or more years.
Discussion
The present study was the first one in Portugal to apply a model to assess the attainment of MI competencies by healthcare professionals, to approach vaccine-hesitant parents. The pre- and post-training survey results showed a significant increase in the participants’ scores in all three pre-defined dimensions: acquisition of knowledge, perception of skills application, and sense of confidence. Despite the overall increase in the scores across all dimensions of the MI survey, it is noteworthy to highlight some specific features of the results obtained. In the case of the current Portuguese study, the increment tends to be the smallest of all the studies. Namely, in the MI knowledge dimension, the increase of 11.6 differs substantially from the 21.7 in the research carried out in France 48 and 27.1 in Canada 25. Also, in the skills application, the increase in score of 38.5 points and 21.3 in the French and Canadian cases, respectively, is substantially above the 11.9 in the Portuguese case. The exception to this trend is only in the sense of confidence, where the 18.3 increase in the Portuguese study is above the 11.5 increase in Gagneur et al.’s seminal work - although still below the 28.7 increase in a French study 48. Moreover, it is also in the sense of confidence that the effect size in the present study (1.25) is substantially larger than in previous studies. This scenario differs from the predominant effect size of the training in the MI knowledge dimension (1.66) observed in the precursor study by Gagneur and colleagues 25 - the only effect qualifiable as very large 50,51. It is substantially different as well from the flattening tendency of approximately 0.8 across all dimensions in the case of the research on a French study 48. Regardless of these dissimilarities, the results reinforce those obtained in the two studies mentioned above regarding the impact of MI training.
When comparing the different studies using the MISI tool, important differences in the methodological protocol can be highlighted. Firstly, the contents of the Quebec Training Protocol 25 included a practical demonstration followed by an exercise to develop MI-vaccination-specific skills. In the case of the present study, the representation of the MI applied to VH was portrayed through a graphic novel based on the graphic medicine tool. This methodological option may have yielded some advantages, such as the representation of nurses’ and parents’ feelings and thoughts throughout their interaction 6. Secondly, in both the Gagneur and colleagues 25 and Mitilian and colleagues 47 studies, the results were obtained from MI training phases carried out over a more extended time: a 2-month interval, with the MISI survey, applied after each session to assess the evolution in the scores obtained. In the present research, the training program was more limited in time. Notwithstanding, if research suggests the importance of training protocols extended in time in the effectiveness of assimilating the principles and practices converging with MI 19, previous research has also demonstrated the effectiveness of shorter MI training sessions in coaching health professionals 15,27,37. Furthermore, the overall increase in the scores obtained between the pre- and post-training surveys presented in this article suggests that MI training seems to be a promising avenue to pursue to promote healthcare professionals’ communication skills in addressing VH. Thirdly, in the present study, the MISI survey was applied during the training sessions - immediately before and after the training took place. This differs substantially from the procedure adopted in other studies where participants were provided with the MISI questionnaire 2 weeks before and after the training sessions took place 52. Therefore, the application of the MISI questionnaire immediately after the second session of the training may have had an impact on the trainees’ commitment to answering the questions due to tiredness. This may possibly explain the lack of data regarding the open-ended response, jeopardizing the assessment of participants’ application of MI skills in a real-life dialogue. Lastly, concerning the effectiveness of the training, it is necessary to note that participants were recruited voluntarily. As MI involves a set of skills aimed at addressing patients’ ambivalence and finding the motivation to change, rather than strategies based on standardized procedures 15, the effectiveness of the training may depend more heavily on the effective involvement and motivation on the part of the participants. In addition, as in the two previous studies using the MISI tool 25,48, the evaluation protocol does not include an assessment of trainees’ actual communication skills in practice - a limitation identified in other studies of the effectiveness of MI training 37. Furthermore, meta-analyses suggest that maintaining MI skills over time is a challenge that may require ongoing supervision or regular sessions to reinforce learning 29,37.
Notwithstanding the promising results of this MI training, the study’s design encompasses validity limitations as it did not include a control group. This methodological option stemmed from the difficulty of getting healthcare professionals to take part in research, given their heavy workload and limited time available. Future studies should overcome this limitation by adopting an experimental design and randomly distributing the participants over different conditions. This will allow the differences in pre- and post-questionnaire results to be attributed to MI training and not to external factors. Another limitation of the present study is the use of a self-report measure as participants’ answers could be biased due to social desirability reasons. Future studies should employ more implicit measures to assess participants’ MI skills, such as video and audio recordings of real or simulated vaccination encounters 53. Moreover, participants were not asked about their professional role in the questionnaires, not allowing us to distinguish between physicians and nurses working in the context of childhood vaccination. While this methodological option was taken to preserve the anonymization of the participants, it limits a more detailed characterization of the sample. Finally, the described features of the training protocol are also important to contextualize the results obtained and their discrepancies with other studies using the MISI questionnaire as a measurement tool.
On the one hand, about the dimension of confidence, with the highest average score, we must consider the specificities of the training protocol. In particular, the mentioned more compact training period compared to previous studies may have contributed to a lower mean score in the dimensions concerning theoretical knowledge and perception of practical abilities. Another contributing factor is that the post-questionnaire was administered immediately after the end of the training, with less time for the participants to reflect and mature on the content delivered. Therefore, the higher average score in confidence may be associated with a still introductory understanding of the implications of effectively using MI as a communication style, contributing to a reported level of confidence in using an MI-compliant approach above that observed in other studies.
On the other hand, the fact that the mean score for skills was higher than for knowledge may also be associated with the use of communication techniques when approaching patients about vaccination that still lacks reinforced theoretical support to consolidate the use of these practical skills in a clinical context. Regarding the psychometric properties of the MISI questionnaire, the consistency and reliability tests in this study suggest that, in future applications, this questionnaire may require specific adaptations to the particularities of the Portuguese context, especially in the case of the MI skills.
To the best of our knowledge, this was the first study in Portugal assessing the impact of a training aiming to promote healthcare professionals’ immunization-related communication skills based on the MI principles. At the end of the training, participants showed a greater knowledge and perception of MI communication strategies to deal with parents’ doubts or concerns regarding their children’s immunization. Moreover, they expressed a greater sense of confidence when envisioning possible future encounters with vaccine-hesitant parents. Unlike previous vaccination-specific workshops focusing only on MI training 48, the present training also included an initial reflection on the prevailing paternalistic model of communication and how it fuels VH. We think that the contrast between this approach and the patient-centred one allowed us to emphasize the relevance of key MI skills such as asking open questions, empathy, and active listening. Although the positive outcomes of this training, there is evidence showing that MI competencies tend to decrease over time when not applied. This limitation could be possibly minimized by providing support or supervision on an ongoing basis 54. Our results suggest that the integration of MI training in healthcare professionals’ curriculum appears to be a promising avenue to pursue to foster their immunization-related communication skills in Portugal and elsewhere.
Statement of Ethics
Ethical approval was obtained from the Instituto de Ciências Sociais da Universidade de Lisboa (Ref: 2021_16). Informed consent was obtained from all subjects involved in the study.
Author Contributions
Conceptualization: Author 1 and Author 3. Methodology: Author 1 and Author 3. Formal analysis: Author 2. Writing: Author 1, Author 2, and Author 3. Project administration: Author 3. Funding acquisition: Author 3. All authors have read and agreed to the published version of the manuscript.

