











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Food insecurity (FI) is associated with poor health outcomes, higher risk of chronic diseases, and inadequate disease management, with a clear relationship between the severity of FI and health status 1,2. In the presence of chronic diseases, households often face significant financial burdens, forcing them to prioritize basic and essential needs such as food, heating, or housing. In turn, the extreme material deprivation associated with household FI, particularly severe FI, has been associated with compromised food intake and higher stress levels, reducing the ability to manage health problems, and increasing the need for health care 3-5.
Regardless of other social health determinants, household FI is a strong predictor of healthcare utilization and costs among working-age adults 1. The healthcare community increasingly acknowledges the association between social needs of the population, such as FI and housing instability, and health outcomes and costs. Interventions addressing patients’ social needs have been shown to produce improved health outcomes and reduced healthcare expenditures. Therefore, systematic FI screening in healthcare is imperative to meet the social needs of at-risk populations and enhance health outcomes 6-8.
The COVID-19 pandemic, coupled with economic downturns, has contributed to the increased prevalence of FI 9. While 2021 marked a partial recovery from the impact felt, the emergence of the Ukraine war in February 2022, involving two of the world’s major agricultural producers, caused shockwaves in the markets, further increasing uncertainty, and impeding job and income recovery. In many countries, the overall rise in inflation occurred in combination with a decrease in disposable income, prolonging the effects of the pandemic and exacerbating existing inequalities. These events placed an increased burden on the most vulnerable families 10,11.
In 2020, 13.5% of the Portuguese population experienced material and social deprivation, with 18.4% at risk of poverty, and 16.4% reporting reduced family income 12. In addition, the restrictions associated with the pandemic, such as lockdowns and remote work, have led to major changes in consumer behaviors, resulting in income loss and difficulties in affording money 13. FI is identified as a complex and multidimensional phenomenon associated with inequalities in healthcare access and outcomes, especially affecting vulnerable groups such as those in disadvantaged socioeconomic categories (unemployed or in precarious employment conditions, with low education, or income levels) and the elderly population 14,15,16.
The resident population of Amadora municipality is persistently affected by significant fluctuations resulting from migratory flows, with immigrants accounting for 11.2% of the total population in 2016, with 99 different nationalities 17. Compared to the national average of 6.7% immigrant population, Amadora stands out as one of the most culturally diverse municipalities in the country, with the majority originating from African countries, particularly Portuguese-speaking nations 17,18.
Therefore, Amadora’s health status is heavily influenced by demographic indicators, including an aging population, high population density, a large immigrant population, low family incomes, and high unemployment rates 18. Given the national economic picture, the municipality’s demographic characteristics, and the pivotal role of primary healthcare in assessing the food situation of the population, this study was carried out to evaluate and describe the FI status of the primary healthcare population in the municipality of Amadora.
Materials and Methods
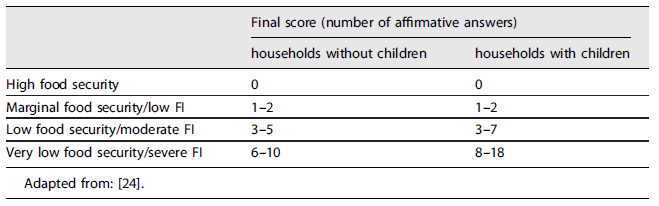
A cross-sectional study was conducted, involving individuals aged 18 and above, living in Amadora for at least 1 year, and attending one of the 10 primary health care units in the municipality of Amadora between April and November 2023, who agreed to participate by giving their informed consent. Sample size was determined using Epi Info™, considering a target population of 179,165 individuals, an expected FI prevalence of 30% 19,20, and a 95% confidence level (CI). Convenience sampling was used, stratified by health unit, to ensure proportional participation from all 10 units of the primary health center. Exclusion criteria included living in institutions and having any physical or cognitive impairment that impeded interview participation. Two intercultural mediators were included in the data collection team to facilitate communication with immigrant participants. They were previously trained in the conduction of the questionnaires and interviews, to minimize observation bias. The interviews took place in designated spaces (meeting or consultation rooms) and comprised two questionnaires. The first questionnaire consisted of closed-response items regarding gender, age, weight, height, nationality, marital status, education, occupation, household composition, and monthly income. Self-reported weight and height were used to calculate the participants’ body mass index, classified according to the criteria of the World Health Organization 21. Household composition referred to the number of people living in the same household, regardless of family relationships. Subjective classification of current health status and smoking habits were also gathered. The second questionnaire assessed FI using a Portuguese-adapted version 22 of the US Department of Agriculture (USDA) Household Food Security Survey Module questionnaire 23,24. A score ranging from 0 to 18 was obtained according to the total number of affirmative answers. Each score was used to assign the respondent to one of four categories of FI (i.e., high food security, marginal food security/low FI, low food security/moderate FI, and very low food security/severe FI) (Table 1). Households with high and marginal food security were classified as “Food secure,” while households with low and very low food security were classified as “Food insecure.” The study protocol was reviewed and approved by the Ethics Committee for Health of ARSLVT.
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) version 28.0, with a significance level of 0.05. Descriptive statistics were used to analyze sociodemographic and health status characteristics. The chi-square test of independence was used to verify the existence of an association between nationality and sociodemographic and health status variables. Spearman’s correlation test was used to assess the correlation between FI level and ordinal variables. The predictive ability of FI for each of the independent variables under study was investigated using binary logistic regression, considering the presence of FI as the event. The selected method for introducing the variables was Stepwise Backward LR, to explore the most useful independent variables in predicting FI, eliminating superfluous ones (25, 26). The results were presented as odds ratios (OR), adjusted ORs, and 95% CIs.
Results
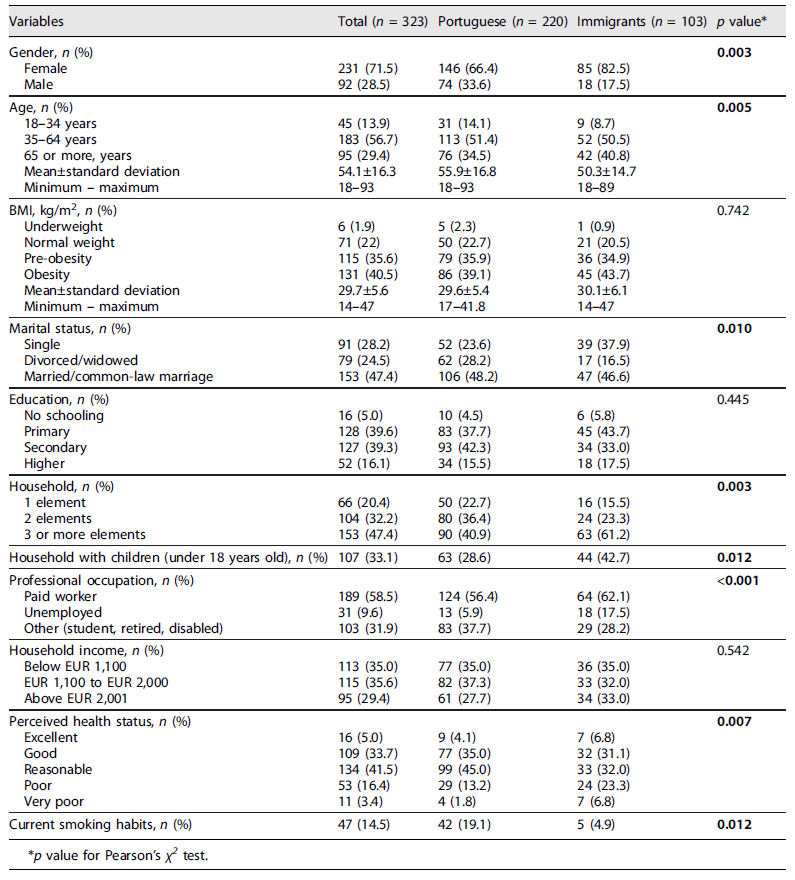
Of the 352 individuals invited to participate, 323 agreed to participate, yielding a high adherence rate of 91.8%. The sample consisted of 71.5% women, with a mean age of 54.1 years (SD: 16.3 years, range: 18-93 years), and included 32% immigrants from 12 different nationalities. Overweight (pre-obesity and obesity) was prevalent in 76.1% of the sample. Nearly half (47.4%) of the participants were married or in common-law relationships, with households consisting of 3 or more members, and 33% had children under the age of 18. Regarding the level of education, 16.1% had completed higher education, while 5% had no schooling. Employment status varied, with 6% of Portuguese participants and 17.5% of immigrants being unemployed at the time of data collection (p < 0.001). Regarding monthly income, 35% of households had an income below EUR 1,100. Smoking habits were reported by 19% of Portuguese participants compared to 4.9% of immigrants (p = 0.012). Almost 20% of the total sample considered their health as poor or very poor, with a higher prevalence among immigrants (p = 0.007). The results for sociodemographic and health status characteristics are presented in Table 2.
Table 2 Sociodemographic and health related characteristics of Portuguese and immigrant participants
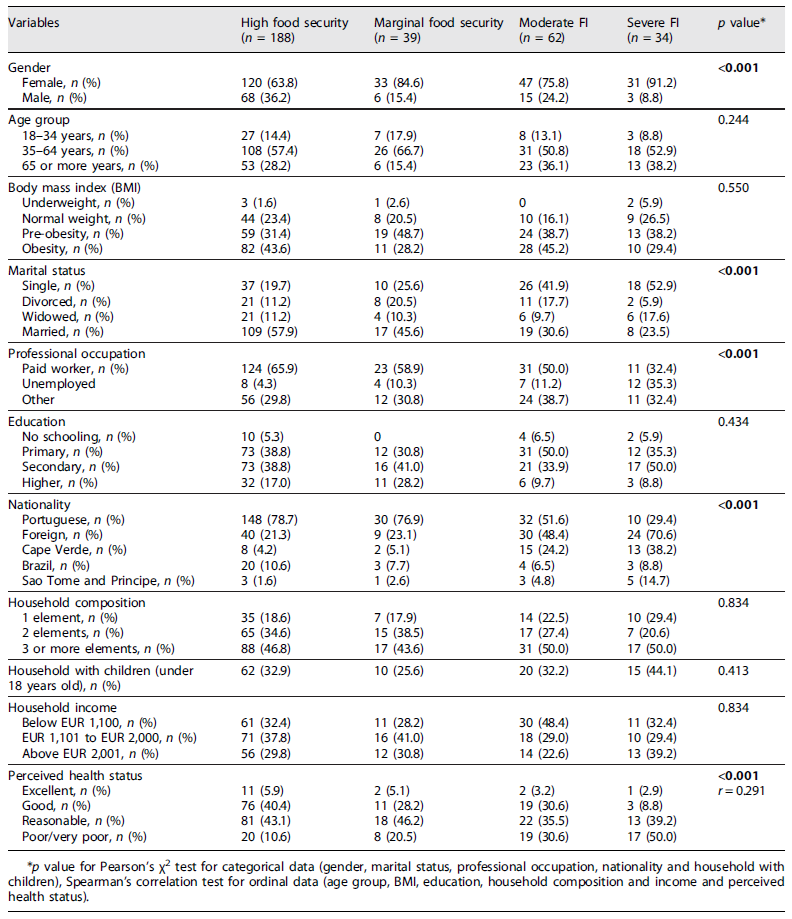
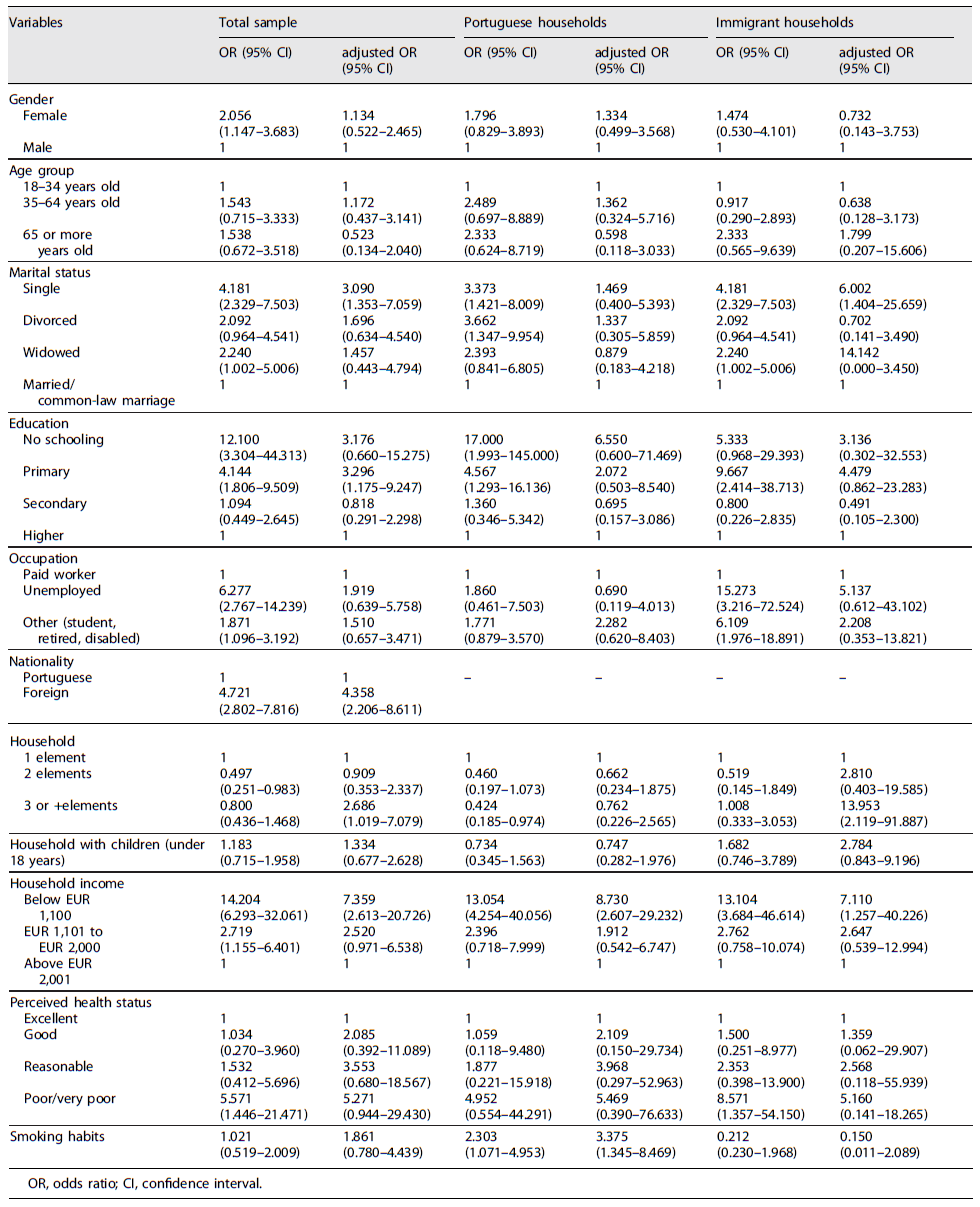
FI was present in 29.7% of households, with 19.2% experiencing moderate FI and 10.5% severe FI. Belonging to FI households was more commonly reported by women (p < 0.001), single individuals (p < 0.001), unemployed participants (p < 0.001), and immigrants (p < 0.001). FI level was also significantly correlated with self-reported health status (r = 0.291; p < 0.001), indicating that poorer individuals perceived health was associated with higher FI levels (Table 3). As shown in Table 4, in the general sample, single participants (OR: 3.090; 95% CI: 1.353-7.059), those with lower education (≤4 years of schooling; OR: 3.296; 95% CI: 1.175-9.247), immigrants (OR: 4.358; 95% CI: 2.206-8.611), households with 3 or more members (OR: 2.686; 95% CI: 1.019-7.079), and households with incomes below EUR 1,100 (OR: 7.359; 95% CI: 2.613-20.726) were more likely to belong to FI households. When evaluating nationalities separately, it was found that FI determinants for Portuguese participants were monthly household income and smoking habits: a household with an income below EUR 1,100 was 8.7 times more likely to be food insecure (OR: 8.730; 95% CI: 2.607-29.232), and participants with smoking habits were 3.4 times more likely to belong to food-insecure households (OR: 3.375; 95% CI: 1.345-8.469). As for immigrant participants, the determinants of FI were marital status (OR: 6.002; 95% CI: 1.404-25.659), household size (OR: 13.953; 95% CI: 2.119-91.887), and household income (OR: 7.110; 95% CI: 1.257-40.226), with single participants, households with 3 or more members, and incomes below EUR 1,100 being more likely to experience FI (Table 4).
Discussion
This study aimed to characterize the situation of FI in the Amadora community. The sample consisted of 323 participants and their respective households registered at Amadoraʼs primary health care center. At the time of this study, the extent of this situation in the municipality of Amadora was unknown.
Sociodemographic Characteristics
As for gender, the sample consisted mostly of women (71.5%), exceeding the percentage reported by the 2021 Census (53.7%), possibly due to women’s higher tendency to use health care services (25). The prevalence of participants in both married or common-law marriages (47.4% vs. 47.1%) and households with two members (32.2% vs. 33.4%) are in line with the city’s demographics 17. Although the immigrant population prevalence was recorded at 13.8% in 2021 (26), 32% of the participants in this study were immigrants, possibly due to the greater use of healthcare services given their significant perception of poor and very poor health status. Education-wise, there was a higher illiteracy rate (5% vs. 2.4%), a higher rate of basic education (39.6% vs. 18.2%), and a lower prevalence of higher education (16.1% vs. 21.9%) compared to the city’s 2021 data 17.
Prevalence of Food Insecurity
The results of this study revealed a FI prevalence of 29.7% among households registered at Amadora’s primary healthcare center, of which 19.2% experienced moderate FI and 10.5% severe FI.
When examining the large nationwide studies carried out in Portugal over the last few years, a significant variability in the prevalence of FI is evident 19,20,26-28. The first exploratory study on FI in the Portuguese population was conducted in 2003, revealing a prevalence of 8.1% 26. In 2005-2006, the Fourth National Health Survey 27 estimated a FI prevalence of 16.5%, with 3.5% of the population facing severe FI. The INFOFAMÍLIA study 19, conducted between 2011 and 2014 among primary healthcare users, reported even higher numbers, suggesting that 48.7% of households were food insecure, of which 10.9% were experiencing severe conditions. Similarly, the IAN-AF study conducted between 2015 and 2016 20, which assessed FI levels among the Portuguese population, found a FI prevalence of 10.1%, of which 2.6% was moderate or severe FI. At the same time, the Epidemiology of Chronic Diseases Cohort Study 27 reported that 19.3% of the adult Portuguese population faced FI, with 1.8% experiencing severe conditions. More recently, during the COVID-19 pandemic, the REACT-COVID study 28 reported that 29.1% of the population was at risk of FI. The reality of FI observed in Amadora can only be compared with the national scenario reported in the IAN-AF study, with its estimated prevalence of moderate and severe FI being more than ten times higher than the 2015-2016 results (29.7% vs. 2.6%). In both, the present study and the IAN-AF study, the full version of the Portuguese adapted scale from the USDA Household Food Security Survey Module, comprising 18 items and specific questions aimed at households with children under 18 years old, was used 22. While differences in prevalence may be due to sociodemographic characteristics specific to the population of Amadora, factors such as the COVID-19 pandemic, the war in Ukraine, food and energy crisis, inflation, and increased debt, all contributing to prolonged economic fragility in the country, may also justify for the rise in FI prevalence compared to 2015-2016 29.
Relation between Sociodemographic Characteristics and Food Insecurity
In line with existing literature, marital status (30, 31), level of education 30,32,33, nationality 14, household composition 31, and income (20 32) are potential predictors of FI. Regarding nationality, immigrant participants and households have a higher prevalence of FI compared to those with Portuguese nationality (OR: 4.358; 95% CI: 2.206-8.611), with Cape Verde and Sao Tome and Principe being the nationalities that most contribute to this disparity. These findings are in line with international data, indicating a strong correlation between race/ethnicity and FI, with black households experiencing higher levels of FI compared to Caucasian ones 34. At a national level, according to IAN-AF data, immigrant populations show a higher FI prevalence compared to the Portuguese population, particularly among non-European countries 14. At a local level, data from Amadora may help explain this discrepancy, since, compared to the rest of the immigrant population, people from Cape Verde and Sao Tome exhibit higher rates of unemployment and precarious housing 18. Moreover, following the COVID-19 pandemic, FI among immigrant populations has been exacerbated, mainly due to job losses, reduced working hours, and low incomes, leading to a reduction in the purchase of nutritionally adequate foods, dietary changes, meal skipping, consumption of cheaper, lower quality food, and prioritization of children’s nutrition 35.
Regarding education, participants with basic education were 3.3 times more likely to experience FI compared to those with higher education (OR: 3.296; 95% CI: 1.175-9.247). These results are in line with those observed by Álvares and Amaral 32, where schooling was the strongest independent factor associated with FI, with individuals lacking formal education being 8 times more likely to experience FI compared to those with a minimum of 10 years of schooling. Aguiar et al. 33 also assessed FI during the COVID-19 period and similarly found that schooling is a crucial social determinant not only of health but also of FI, with individuals with less than 12 years of schooling being 3 times more likely to experience FI. Both in the total sample and the nationality subgroups, income was the greatest determinant of FI, with households with monthly incomes below EUR 1,100 exhibiting ORs between 7 and 8, a trend supported by several studies 14,30,32,33,35, regardless of household composition. However, it should be noted that FI is not exclusive to low-income households, as it also affects other income classes, underscoring that income alone does not fully explain the situation of FI 36. One possible explanation could be based on financial management skills, as households that show greater skills in this area are less likely to experience FI, even among those living with incomes below the poverty line 37. Nutritional education for these households could be a possible strategy since studies indicate that food and nutrition education significantly improves the food security status of low-income families 38,39. Although gender has not been shown to be a good predictor of FI, it is associated with FI levels and is more prevalent among female participants, a trend that has also been reported by other authors 27,31-33,40. This gender disparity can be explained by the fact that the sample had a higher representation of women compared to men (71.5% vs. 28.5%), possibly due to their increased use of health services 25. Even though women contribute to food security at the household level through food acquisition, improved economic access through additional income, and time/food management skills, it has been shown that female-headed households are more likely to experience FI compared to male-headed households 41. This gender disparity appears to be influenced by household composition rather than individual characteristics, with marital status potentially playing a role in cases of poor social relations, suggesting the significant role of having a partner 31. Although no significant association between gender and marital status was observed in the study sample (p = 0.160), there was a weak but significant correlation between marital status and household composition, with most participants from households comprising of more than two individuals being married or in common-law marriage (r = 0.236; p < 0.001). Moreover, marital status was one of the predictors of FI, with single participants (86% of whom were women) being three times more likely to experience FI than those who were married or in common-law marriage (OR: 3.090; 95% CI: 1.353-7.059).
Relation between Health Status and Food Insecurity
In terms of perceived health status, 18% of the total sample considered their health as poor or very poor, a factor significantly correlated with FI levels since 50% of severely food insecure participants classified their health status as poor or very poor (r = 0.291; p < 0.001). Self-perceived health status is a valid and efficient measure of mental and physical health. It is comparable to other more complex instruments and can be used as a predictor of mortality, hospitalizations, and high use of outpatient services 42,43. Smoking was reported by 14.5% of the participants and was associated with nationality, with a higher prevalence of smokers (89%) in the Portuguese population (p = 0.012). Smoking was found to be a determinant of FI in this subgroup, with smokers being 3.4 times more likely to belong to a food-insecure household than nonsmokers (OR: 3.375; CI: 1.345-8.469).
Although 39.6% of food insecure participants were obese, no significant correlation was found between body mass index and FI (p = 0.550). This could be due to the high prevalence of obesity in the studied sample (40.5%), which exceeds the national figures of 22.3% observed in 2015-2016, and can be explained by the high rate of primary healthcare use among overweight individuals 44. The coexistence of both FI and obesity is referred to as paradoxical since it seems contradictory: while FI results from a lack of economic means to access food, obesity results from excess energy compared to energy expenditure 45. Hypotheses studied to explain this paradox include the consumption of high energy-dense and hyper-palatable foods in food-insecure populations, insufficient nutrition knowledge, limited resources, and lack of access to healthy, affordable foods 46,47. Since poverty is a key factor that contributes to FI and directly triggers the consumption of unbalanced diets, without essential nutrients, in low- and middle-income populations, FI and poverty not only contribute to an increase in malnutrition, but also in the prevalence of obesity, with an increased risk of sarcopenic obesity 45,46.
Conclusions
This study revealed a significant prevalence of FI within the community, estimated at 29.7%, of which 10.5% experiencing severe FI and 10.8% living in households with minors. FI status was found to be associated with gender, marital status, professional occupation, nationality, and perceived health status. Potential predictors of FI include being single, having basic education, being an immigrant, living in a household with three or more members, and having an income below EUR 1,100. Among immigrants, those in larger households, unmarried individuals, and those with lower incomes appear to be the most vulnerable groups, while among the Portuguese population, smokers and households with low incomes are at greater risk of FI. Consequently, it should be a priority to raise awareness of the FI as a persistent symptom of inequality, necessitating monitoring at both national and regional levels to identify needs and target community intervention.
Study Limitations
The study’s cross-sectional design limits the ability to draw causal and temporal inferences about the association between the studied variables. Additionally, the non-random sampling method may not accurately reflect the true patterns of the population of Amadora. Also, self-reported data is subject to social desirability bias; as FI is a sensitive topic, participants may omit information about their reality, leading to an improper classification of their food security situation. Memory bias may also be present, as the assessment of FI refers to the 12 months prior to the study date. However, despite these methodological limitations, a validated instrument was used under similar conditions, and all data collection was carried out consistently by a properly trained team.
Implications for Practice
The findings of this study offer valuable insights into the sociodemographic and health status factors associated with FI among individuals living in Amadora, allowing us to understand which households are at higher risk. To the best of our knowledge, this is the first study to estimate FI prevalence in Amadora. Given that improving the quality of life and well-being is a priority in Amadoraʼs Social and Health Development Plan for 2018-2025, particularly focusing on promoting healthy lifestyles and addressing the high incidence of diseases associated with poverty factors in vulnerable groups, the results underscore the urgency of integrated community programs that include health and social action 18. Enhancing food literacy is crucial, especially among identified vulnerable groups, while taking into account cultural aspects that influence food utilization, choice, and allocation within the households.
Acknowledgments
The authors thank Asmila Balde and Jocilene Moreno from AJPAS - Community Intervention, Social and Health Development Association - for their collaboration in interviewing immigrant participants.
Statement of Ethics
The protocol of the study was previously reviewed and approved by the Ethics Committee for Health of ARSLVT, with the Approval No. 1072/CES/2023. Written informed consent was obtained from all participants in the study.

