











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
According to World Health Organization (WHO), quality of life assesses individuals’ perceptions of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns 1. It is a complex concept that includes health and psychological well-being dimensions 2. As follows, one of the fundamental factors that positively influences quality of life is good mental health. Concerns about children and adolescents’ mental health continue to increase despite more awareness into the issue.
According to data provided by Global Health Data Exchange, it is estimated that 1 in 7 children aged 10-19 years’ experience mental health conditions worldwide. Nevertheless, these remain unrecognized and untreated in many cases 3. The most common mental health conditions in adolescents are anxiety disorders. It is estimated that 3.6% of 10- to 14-year-olds and 4.6% of 15- to 19-year-olds experience anxiety 3. Depression is estimated to occur among 1.1% of adolescents aged 10-14 years, and 2.8% of 15- to 19-year-olds 3. In Portugal, most adolescents consider themselves happy (81.7%), but from those who do not feel as happy, about 27.6% feel worried several times a day, every day 4. Also, Portuguese adolescents feel nervous (13.6%), irritable (12.6%), sad (9.2%), and afraid (6.3%) daily 4. Adolescents who suffer from mental health conditions are particularly at risk for social exclusion, discrimination, stigma (affecting readiness to seek help), educational difficulties, risk-taking behaviours, physical ill-health, and human rights violations 3. On the other hand, children and adolescents who are happy and confident are more likely to reach adulthood with a better quality of life and show higher resilience towards hardship 5. Early assessment, intervention, and promotion of positive mental health may empower young people as they develop into adults.
The five-item World Health Organization’s Well-Being Index (WHO-5) is a short and generic global rating scale, derived from WHO-10 by the Psychiatric Research Unit, Mental Health Centre North Zealand, Hillerød, Denmark 1,6. This scale was designed to measure psychological well-being, has adequate validity both as a screening tool for depression and as an outcome measure in clinical trials, and has been applied successfully as a generic scale for well-being across a wide range of study fields (6). Nevertheless, this scale has been used extensively in adults, and only a few studies were published in the paediatric population 7-11. Since its publication in 1998, it has been translated into more than 30 languages and used in research studies globally (1, 6‒10). The Portuguese version was developed by the same group who designed the original scale and is available online 12. Although previously applied to adolescents in Portugal, the psychometric properties of this version have not yet been examined in that specific population 9-11,13.
The main purpose of this study was to analyse the psychometric properties of the Portuguese version of the WHO-5 well-being index in a Portuguese adolescent population. The scale construct validity, internal consistency, and unidimensional structure were assessed. Another aim was to assess the relationship between psychosocial traits and general well-being.
Materials and Methods
Study Design and Sample
We performed a post hoc analysis on a study that was aimed at assessing adolescent internet addiction and the role of parental control 9. This cross-sectional survey-based study was conducted in a regional subset of Portugal (Cova da Beira) and included adolescent students attending public schools. Both elementary and secondary schools, accounting for 3,788 students from grades 7 through 12, were invited to participate. A total of 1,916 eligible responses were obtained.
Instrument
The questionnaire comprised three sections: (1) questions on sociodemographic factors, health-related aspects, and lifestyle habits; (2) a validated scale assessing the risk of internet addiction; (3) the WHO-5 scale for well-being. The WHO-5 scale only has positively worded questions. Measuring positive well-being rather than depressive symptoms is more gainful since it is considered better accepted by patients and more effective in detecting depression 14 The respondents were asked to rate how well each item applied to them in the last 14 days. Each of the five items could be scored from 0 (“none of the time”) to 5 (“all of the time”). The final score was obtained by adding the five individual scores, with results ranging from 0 to 25. A score below 13 suggests poor well-being 1,12,15 and is an indication for testing for depression 1,15.
Procedure
Approval by the Portuguese Ministry of Education and the Portuguese Data Protection Authority was obtained before the study. Written consent was obtained from all participants or, where relevant, from their legal guardians. Participants answered a questionnaire under their class teacher’s supervision. Respondents with unsigned consent forms and participants older than 17 years and 365 days were excluded from the study. Data collection was performed between September and October 2017.
Statistical Analysis
General sociodemographic, psychosocial traits and behavioural data were collected for the main study, detailed and discussed in a previous publication 9. For this secondary analysis, we examined the WHO-5 questionnaire scores alongside data on age, sex, medical history, and social behaviours. Specifically, we focused on participant’s ability to make friends easily, their engagement in sports, and any reported sleep problems. The independent samples of the t-test were conducted to compare groups. Emotional well-being was scored using the Portuguese version of the WHO-5 (shown in online supplement 1; for all online suppl. material, see https://doi.org/10.1159/000543728) 12.
We used confirmatory factor analysis (CFA) to test the structure of the construct WHO-5. Parallel analysis was used to identify the number of dimensions/factors to retain in principal component analysis (PCA). We used PCA for categorical variables, which allowed us to produce numerical values for PCA and reduce our data’s dimensionality. We used the minimum average partial method to achieve the same goals for redundancy. The unidimensionality of the WHO-5 scale was tested with parallel analysis 16,17 and the minimum average partial method 18-20, complemented by a principal component analysis for categorical variables 21.
CFA for categorical variables was conducted since the present study aims to validate a hypothesized measurement model 22. The analysis was performed with version 4.2.1 of the software R 23 using packages Lavaan version 0.6.12 24, psych 25, and semPlot 26. Model fit was assessed by goodness of fit measures - Goodness-of-Fit Index (GFI), Incremental Fit Index (IFI), Tucker-Lewis index (TLI), with a cut-off value close to 0.95 or above 27, and badness of fit measures - root mean square residual and root mean square error of approximation (RMSEA), with cut-off values below 0.08 and 0.06, respectively 27.
Results
A total of 1,916 eligible responses were obtained. The mean age was 15 years (SD = 1.8), with a slight predominance of female (53%) participants. The median z-score of body mass index was −.24. The WHO-5 median score in our sample was 17 (IQR 14-20), with 172 (9%) scoring below 13. A CFA was conducted with a sample size of 1,701 after the case wise deletion of missing data. This size is way above the minimum of 200, which maximizes the decrease in the standard deviation of the RMSEA 28. The model, estimated with maximum likelihood, has ten parameters (q: 5-factor loadings and five measurement error variances), which results in a ratio of 170.1 observations per estimated parameter (N:q), well above the threshold of 10:1 for maximum likelihood estimated models 29. Figure 1 depicts the final model of CFA, which includes five observed variables, five measurement error terms, and one construct, WHO-5. The initial model is shown in online supplement 2.
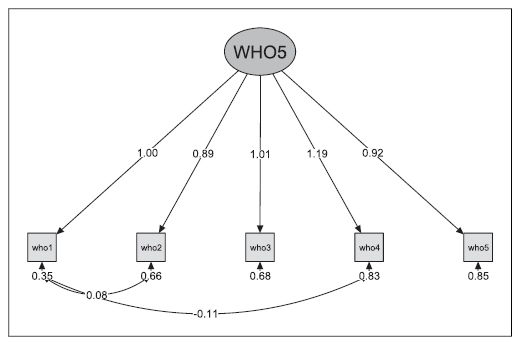
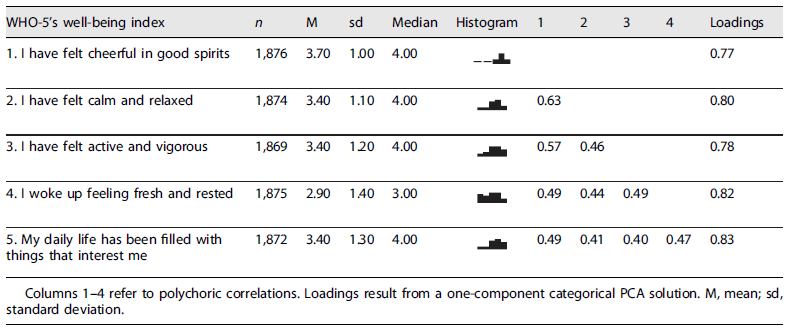
The unidimensionality of the WHO-5 scale in Portuguese was confirmed as parallel analysis, minimum average partial method, and principal component analysis for categorical variables all converged to the solution of one component/factor. Results in Table 1 indicate that most variables exhibit moderate to high polychoric correlations. In this model, all factors loading were good. To further examine the validity of the target model presented in Figure 1, we used CFA techniques to analyse it. Results in Table 2 show that the model fit is slightly outside the acceptable criteria for fit recommended by Schumacker and Lomax 22. As the fit was unsatisfactory, the model was modified 22 based on modification indexes (MI), which measure how much the reduction will be on the discrepancy between the model and data when parameters are added or freed or when equality constraints are relaxed in the model of Sörbom 30. The use of MI must be done with caution, as mentioned by MacCallum and colleagues 31, so MI were not used to change the structural model proposed by theory, allowing only the manifest variables to covary. In the modified model, two pairs of measurement errors were allowed to covary. Table 2 shows that the measures of the modified model reflect a good fit. The Cronbach’s alpha, a measure of internal consistency, was 0.80, consistent with the high internal consistency of the WHO-5 questions. The resulting model with unstandardized parameter estimates is provided in Figure 1.

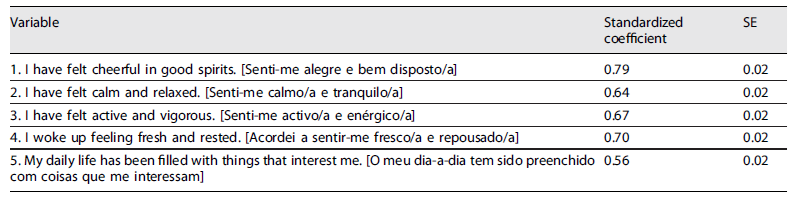
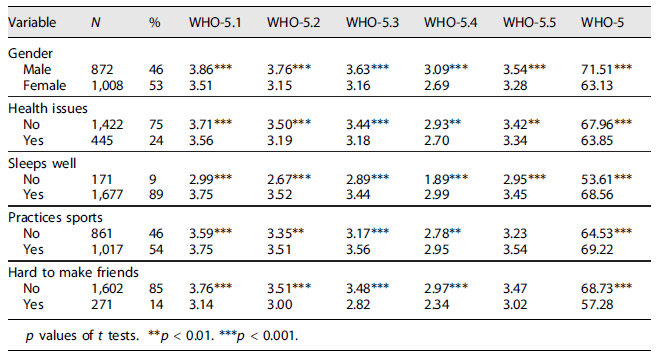
Standardized estimates are presented in Table 3 and standard errors. Overall, the results obtained with the CFA were acceptable and indicated a good fit model, thus showing that the WHO-5 scale is valid for our studied population. As shown in Table 4, the best WHO-5 scores were found in males (p < 0.001), in those with no health issues (p < 0.001), who slept well (p < 0.001), who practiced sports (p < 0.001), and those who had no difficulties making friends (p < 0.001).
Discussion
This analysis of the Portuguese version of the WHO-5 index on a sample of adolescents showed good internal validity, with Cronbach’s alpha value of 0.80. This indicates that the answers for each question are consistent and do not overlap, thus conferring a high internal consistency to this model. Acceptable to high internal consistency was also found in previous studies with clinical and community samples of various age groups 14,32-38. Particularly in the adolescent population, the Cronbach’s alpha values ranged from 0.7 in Ghana 34, 0.78 across several European countries 35, and 0.85 in the Netherlands 36.
The CFA results support the unidimensional structure of the questionnaire, as described by other authors 5,30,31,34,35. After modification, the final model showed good fit measures, with TLI, GFI, and IFI values >0.95 and root mean square residual and RMSEA <0.08. In the PCA, factor loading for the items ranged from 0.77 to 0.83. These results confirm that the WHO-5 has a unidimensional structure, with validity and consistency criteria to evaluate general well-being in Portuguese adolescents.
Adolescence is one of the most formative phases of human development, with selective physical, cognitive, emotional, and social maturation. It is also the time to seek the balance between risky and protective behaviour, personality education, consolidation of social roles, and lifestyle choices. The WHO-5 median score in our sample was corroborated with previous studies conducted in our country 11. To explain the high levels of well-being observed in adolescents, several studies suggest that throughout life, there might be a slight decline in positive affection attributed to the focus on post-materialist goals that favour younger generations 39. However, 9% of adolescents scored below 13, which indicates poor well-being and a potentially higher risk of developing depressive symptoms. Previous studies demonstrated that the WHO-5 had good diagnostic accuracy for depression and could be applied to adolescents 8. Adolescents who test positive may, nonetheless, still need careful diagnostic evaluation for depression 40.
Also, in line with previous studies 8,41, we reported higher WHO-5 scores in male adolescents, which suggests they experience a better well-being state than their female counterparts. Evidence tells us that many reasons may be behind this trend, a significant part of it being due to different stages of development and maturation. Young males start developing their personality more on a personal note, rather than a social one, whereas young females usually prioritize their social sense of identity. Females are also more emotional, have more internalization behaviours 11,39,42, and show reflective mindsets early on. At the same time, male adolescents usually mature later keeping a proactive, externalized, and simpler way of thinking for a longer period 11. The latter may induce a general prolonged feeling of well-being when compared to girls of the same age. Interestingly, these differences in gender characteristics are not constant but rather fluid from adolescence into adulthood, with a tendency to decrease with age 11.
Other important aspects that we reported having better scores in WHO-5 are having no problems in sleeping and practicing sports. Quality of sleep and physical exercise are associated with good health and emotional outcomes during adolescence. Conversely, lack of sleep is often related to poorer health and emotional well-being, with increased self-criticism, internalizing symptoms, and impairment of cognitive functions, among others 43. Regarding physical exercise, a clear benefit in health and wellness has been described in people who are physically active and practice sports. Our study further corroborates these findings with adolescents mentioning the practice of sports having higher scores on WHO-5 when compared to those who do not have sports habits. On another note, we saw that those who mentioned not having problems in befriending others scored higher on WHO-5. It has also been proved that people with a better social network and peer support frequently show better well-being and report a higher level of self-esteem 11. Furthermore, a positive association between social competences and well-being has been reported, with social networking being very important for the natural development of adolescents 44. The development of social competences allows for better establishing a network of friends, which is thought to increase the general well-being of young people 44.
As mentioned before, mental health issues are increasing among adolescents, and as such, it is important to raise awareness of these conditions among physicians who care for children and adolescents, knowing that early detection is crucial for successful management.
Recent evidence suggests that anxiety and depression levels among adolescents have increased in the past few years, mostly after the COVID-19 pandemic 45,46. Also, the WHO-5 median score has been declining in Portugal 47 and worldwide 48. Moreover, in Portugal, some studies reported an increase in depressive symptoms, 11.2% vs. 15.4% before and after the COVID-19 pandemic, respectively 49. Therefore, more than ever, it is imperative to be aware of these problems and have adequate tools to screen them.
Since this scale can be used as a screening tool for depression and as an outcome measure of well-being, there is a growing field of research around it, which can be extended to other population contexts 6,9,10,13. It is also important to highlight that patients who had scores <13 should be further investigated to confirm a diagnosis of depression, to rule out normal distress symptoms, or organic causes for depression.
Limitations and Strengths
Regarding the nature of this study, some limitations must be considered. Results from this research derived from an ad hoc analysis study, which pertained to a larger study on our selected sample population. Moreover, the sample population corresponds to a subset of adolescents from a specific Portuguese region, so generalization must be done carefully. Finally, we must consider response bias since results were based on self-reported surveys by adolescents.
Besides these limitations, some strengths should also be mentioned. We analysed a sample with a considerable size which strengthened our results, contributing to a smaller margin of error and greater accuracy of the results. To the best of our knowledge, this is the first study addressing the WHO-5 properties in Portuguese adolescents.
A few major findings from this study include (1) the positive outcomes of the current study indicate that the wording and response format of the WHO-5, initially designed for adults, is also appropriate for adolescents; (2) a positive association between certain behaviours in adolescence and improved well-being, such as easy socialization, sports practice, or sleeping well; (3) female adolescents appear more susceptible to poorer well-being, likely due to more internalized and emotional behaviour. This pattern seems to be more characteristic in this phase of their lives when compared to male adolescents.
In conclusion, our findings showed good internal consistency and unidimensionality of the WHO-5 for Portuguese adolescents. It also provided an overview of the general well-being of the study population. Fostering healthy habits and lifestyles in adolescents can be impactful in their well-being and should opportunistically be encouraged by all healthcare professionals. Further implications of our work suggest that the WHO-5 is a simple and readily useable scale that can be applied in routine appointments by family doctors or general paediatricians. It is also a suitable tool that can be used both in clinical practice and research for screening the emotional state of adolescents and early detection of signs of mental health issues.
Statement of Ethics
This study protocol was reviewed and approved by Portuguese Ministry of Education and the Portuguese Data Protection Authority before the beginning of the study. Written consent was obtained from all participants or, where needed, from their legal guardians to participate in the study.
Author Contributions
Paula Saraiva Carvalho, Miguel Vieira Martins, and Sofia Ferreira designed the experiments. Paula Saraiva Carvalho, Miguel Vieira Martins, and Isabel Azevedo wrote the first draft with contributions from Sofia Ferreira. Miguel Vieira Martins and Sofia Ferreira collected the data. Ricardo Rodrigues analysed the data. All authors reviewed and contributed to the subsequent drafts of the manuscript. All authors approved the final manuscript.

