











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkA 41-year-old healthy man presented with a 2-year history of asymptomatic, progressively enlarging lesions on the external aspect of the left thigh. Its onset could not be correlated with trauma, medication or contact with any substance. On examination, two reticulated brownish well-defined patches, with 1 and 1.5 cm in diameter, were observed (Fig. 1A). Biopsy showed a superficial dermal dense, band-like lymphocytic infiltrate accompanied by scattered extravasated erythrocytes (Fig. 2B). A Perls’ stain highlighted the hemosiderin deposition (Fig. 2C). It was consistent with lichen aureus (LA).
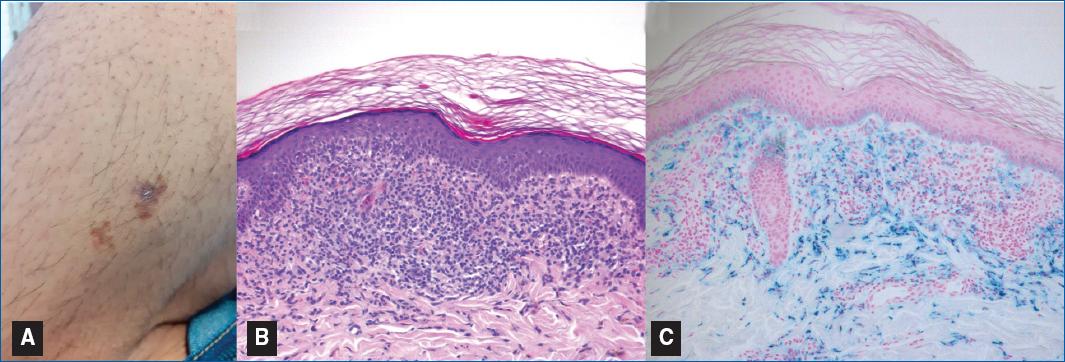
Figure 1 Lichen aureus. A: clinical picture of two reticulated brownish patches on the thigh. B, C: histopathologic picture revealing a lichenoid infiltrate in the upper dermis with erythrocyte extravasation and hemosiderin deposition evidenced by Perls’ stain (B. H&E, x100; C. Perls’ stain, x100).
Lichen aureus is a rare variant of pigmented purpuric dermatoses (PPD), occurring mainly in childhood1. Although its etiology remains unknown, its pathogenesis seems to be related to inflammation and hemorrhage of superficial papillary dermal vessels, usually capillaries2. It clinically presents with persistent asymptomatic golden to brown colored macules and patches, usually on the lower limbs, with a unilateral distribution2,3. Dermoscopy can be useful showing brownish or coppery-red amorphous area, red dots and globules, gray dots and a network of brownish to gray interconnected lines2,3. The definitive diagnosis is based on histopathology, with characteristic findings described in the reported case1-3. The therapeutic arsenal includes PUVA, calcineurin inhibitors and corticosteroids, frequently with unsatisfactory results3. Patients should be reassured regarding the benign and chronic nature of the condition.

